CNS Response, Inc.
There are over 100 medications available for treatment of behavioral
disorders. The core problem is not that we need three more. The
problem is we need to know how to use the 100 that we
have.
Stephen Suffin, MD,
Quest Diagnostics
Chief of Clinical Pathology
Co-Founder of CNS Response
October 2007
2
Safe Harbor
The statements and discussions contained in this summary that are not historical facts constitute
forward-looking statements, which can be identified by the use of forward-looking
words such
as “believes,” “expects,” “may,” “intends,” “anticipates,” “plans,” “estimates” and analogous or
similar expressions intended to identify forward-looking statements. CNS
Response wishes to
caution the reader of this summary that these forward-looking statements and estimates as to
future performance, estimates as to future valuations and other statements contained herein
regarding matters that are not historical
facts, are only predictions, and that actual events or
results may differ materially. CNS Response cannot assure or guarantee you that any future
results described in this summary will be achieved, and actual results could vary materially from
those
reflected in such forward-looking statements.
Information contained in this summary has been compiled by CNS Response from sources
believed to be credible and reliable. However, CNS Response cannot guarantee such credibility
and reliability. The forecasts and projections of events contained herein are based upon
subjective valuations, analyses and personal opinions.
This summary shall not constitute an offer to sell or the solicitation of an offer to buy any
securities. Such an offer or solicitation, if made, will only be made pursuant to an
offering
memorandum and subscription documents prepared by CNS Response specifically for such
purposes.
3
Psychiatric Treatment:
General Medical Treatment:
The Problem:
Psychiatry Lacks Physiological Measures
1.
Symptoms
2.
Physiologic measurements
3.
Treat to mitigate pathophysiology
3.
Assess Outcomes
1.
Symptoms (behavior)
2.
Attempt to treat symptoms
2.
Assess Outcomes
“In most branches of medicine, physicians base diagnosis on objective tests: x-rays for broken
bones, examination of tissue samples for cancer cells. But
for some common and serious psychiatric
disorders, diagnoses are still based entirely on the patient’s own report of symptoms and the doctor’s
observations of the patient’s behavior” (Dr. Steven Hyman, Director of National Institute
of Mental
Health, Scientific America, September 2003),– This is the contribution of rEEG.
4
CNS Response Overview:
First to Market a Proven Biomarker System
CNSR has developed and patented technology consisting of a
biomarker system and database to serve the multi-billion dollar
Psychiatric Addiction and Pharmaceutical
Development markets.
Laboratory Services to the Psychiatric Market
“What is the right
medication(s) for my patient”
Proprietary Expertise and Technology for Pharmaceutical Companies
“What patients are right for my medication”
5
What is it?
Introducing Referenced-EEG (rEEG)
Standard Digital EEG
+
=
rEEG
Medical Correlations
+
Analysis[2]
Compare to Stratified Outcomes Database
to Correlate (13,000 treatments, 4000+ patients)
Analysis[1]
Compare to “Normal” Database to Stratify
6
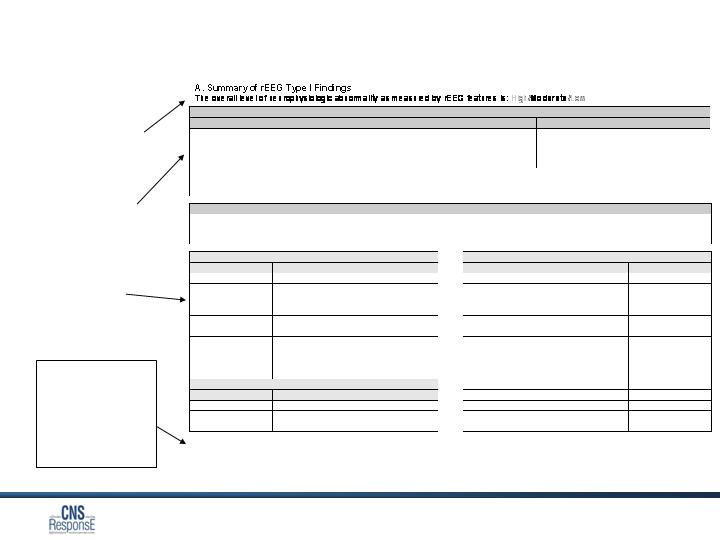
The rEEG Report
Section 1
Comparison with
Outcomes Database to
identify categories of
medications helpful to
similar patients
Section 2
Within categories,
identifies specific
medications helpful to
similar patients
S = Sensitive
R = Resistant
I = Intermediate
1,2,3 = relative
rankings within a
subgroup
Section A
Comparison with
Normal people of
same age and sex
Section 1: Drug Class Correlations
Drug Class
Sensitivity
Biomarker Predominance
Beta Blocke
rs
Sensitive/
Intermediate
/Resistive
High
/Moderate/Low
Anticonvulsants
Sensitive
/Intermediate/Resistive
High
/Moderate/Low
Antidepressants
Sensitive/Intermediate/
Resistive
High/Moderate/
Low
Stimulants
Sensitive
/Intermediate/Resistive
High
/Moderate/Low
C
orrelations are based on a subset of more than 1,600 patients in the rEEG database having (1) similar rEEG features to this patient and (2) a
change of two or more improvement in their Clinical Global Improvement Index (CGI).
Section 2: Individual Medica
tion Responsivity
Subgroup ratings (S, I & R) are based on comparison to other subgroups within the overall medication group. Within the subgroup
individual medications ratings (1, 2, 3) are relative to other medications in the subgroup only. When there i
s only one medication in a
subgroup only the subgroup rating appears. Specific medication combinations may be incompatible.
Anticonvulsants (
Sensitive
)
Stimulants (
Sensitive
)
Trade Name
Generic Name
Sensitivity
Trade Name
Generic Name
Sensitivity
Be
nzodiazepines
R
MAOI
I
Xanax
Alprazolam
Manerix
m
Moclobemide
1
Ativan
Lorazepam
Parnate
Tranylcypromine
3
Klonopin
Clonazepam
Eldepryl
Selegiline
2
Tegretol
Carbamazepine
R
Nardil
Phenelzine
ND
Depakote
Divalproex
S
Ri
talin
Methylphenidate
R
Neurontin
Gabapentin
I
Dexedrine
d
-
Amphetamine
S
Lithane
Lithium
I
Adderall
d,l
-
Amphetamine
R
Gabitril
Tiagabine
ND
Provigil
Modafinil
ND
Beta Blockers (
Intermediate
)
Trade Name
Generic Name
Sensitivity
Lopressor
Metoprolol
I
Inderal
Propranolol
I
Tenormin
Atenolol
I
Key to symbols:
S
=
sensitive
, patients with similar neurophysiology were most often responsive to medications with this designation.
R
=
resistant
, patients with similar
neurophysiology were least often responsive to medications with this designation.
I
=
intermediate
, patients with similar neurophysiology were neither consistently sensitive or consistently resistant to medications with this designation
ND = No data in the
database to support recommendations
1,2,3 = relative rankings amongst agents in a subgroup where 1 is highest and 3 is lowest.
m
-
Available in Canada
Jane Doe’s History &
Treatment >
rEEG was essential to
treatment success >
8
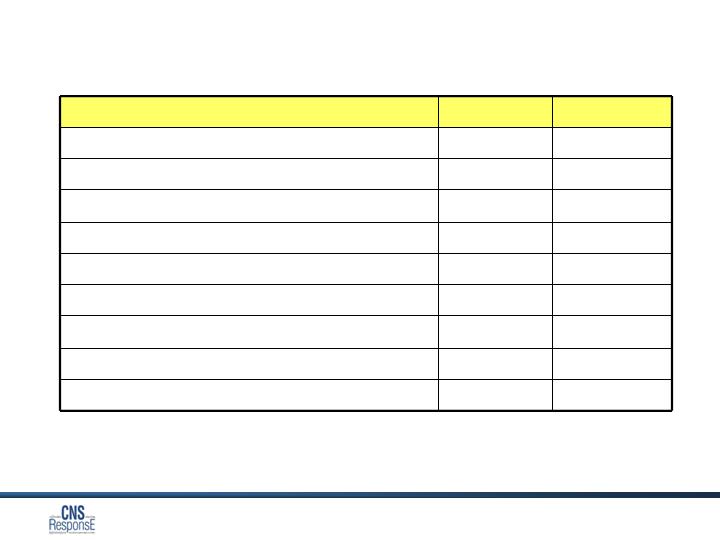
Name
Population
Efficacy
ADD & Depression Trial1,3
100
80%
VA Blinded Study3,5
13
85%
CIGNA-Atlanta Pilot3
56
70%
Dr. Davis Case Series3
15
100%
Monte Nido Case Series2,3
150
80%
Dr. Hamilton Case Series3
34
78%
Dr. Hoffman Case Series3
74
76%
Rancho L’Abri Case Series3,4
58
93%
TOTAL
500
81%
Does it work?
Proven Efficacy in Multiple Studies
1 Clinical EEG and Neurosciences, 1995
2 NCDEU Poster at Annual Meeting 2004
3 APA Poster at Annual Meeting 2005
4 APA Poster at Annual Meeting 2005
5 Accepted for publication Amer College Phys Surg 2007
We have three branches of Intellectual Property:
1. Basic Methods Patent: (# 6,622,036) issued September 2003 and comprising:
Obtaining neurophysiologic information from a patient;
Quantifying the neurophysiologic information and comparing to
Outcomes Database;
Correlating the quantified neurophysiologic information to medication
therapy responsivity profiles, without regard to psychiatric diagnostic
category.
Numerous other active application in this lineage
2.
Electroencephalography based systems and methods for selecting therapies and
predicting outcomes.
(#7177675) issued February 2007
Numerous other active patent applications in this lineage.
3.
Combination Medication Drug Patents:
We have filed three patents surrounding novel combinations of
medications.
Can it be protected?
Two core issued patents
How big is the market?
Lab Services > $1BB per year
Private Pay
Direct out-of-pocket payment by patient.
Represents 34.6% of the 45,000 Psychiatric Practices
Patients will pay out-of-pocket, when: (1) they have exhausted their
benefits; (2) require complete confidentiality; (3) seeking the best
possible treatment.
Target 20-40% of these patients
Managed Behavioral Healthcare Organizations (MBHOs)
Manage 210 million lives in the U.S. alone.
115 million individuals covered by one of four MBHOs:
Magellan, Value Options, United, CIGNA.
Target: 10% of patients account for 35%-40% of medical budget.
VERY expensive med. device treatment options are emerging
(VNS, deep brain stimulation, rTMS)
11
A win-win-win for everyone
Providers
Patients
Payers
1)
Treatment success
where there had been
failure.
2)
Profitable procedure.
3)
Patient retention.
1)
Better results /
Reduced trial and error.
1)
Increased efficiency
and economics.
1)
Dramatic decrease in
patient utilization of
services.
2)
Reduced medication
costs through
increased use of
generics.
12
Pharmaceutical Market Opportunity
Pharmaceutical sales to treat CNS Disorders is the largest such market in the
U.S. with $44 Billion of sales in 2005 ($68 Billion,
worldwide).
Represents 23% of total annual pharmaceutical sales.
Expenditures are not based on any objective test.
Business Opportunity
New drug combinations from off-patent medications
Repurposing - New undiscovered indications
Resuscitation of medications failing clinical trials
Better decision making throughout the drug development process

13
$8MM financing closed March 2007
_________________
Acquisition of first Center of Excellence in Denver
Completion of Thought leader SAB, design and recruited sites for multi-site
trial
Set up China data collection capability
George Carpenter joins as President to lead 2008 commercialization
Daniel Hoffman, MD joins as Chief Medical Officer
Henry Harbin, MD, founder and CEO of Magellan joins BOD
First payer negotiated reimbursement and codes
Newsweek article – demonstrates newsworthiness of rEEG
2007 Key Accomplishments
14
Completion of 11-site academic study in depression
Negotiation of first payer reimbursement and execution of additional payer
pilots
Expansion of network of regional medical directors who are the training
infrastructure and database suppliers.
Addition of antipsychotics to the database.
Implement “while-u-wait” report turnaround
First pharma development application
2008 Milestones
15
Management
Name
Position
Background
Leonard J.
Brandt
Chief Executive
Officer
Co-Founder, CNS Response, Inc.
Partner, Norwest Venture Capital;
George
Carpenter
President
CEO of Core, Inc.-- leading disability mgmt.
companies, CEO of WorkWell Systems, Inc. –
leading worker’s compensation mgmt. company
Daniel
Hoffman
Chief Medical Officer
Medical Director, The Neurotherapy Clinic
Brian
MacDonald
Director of
Engineering
Co-Founder, CNS Response, Inc.
Operations Engineering Consulting, 10 years;
Horace Hertz
Chief Financial
Officer
CEO/COO/CFO, various companies for 11 years
Partner, Deloitte & Touche
16
Directors and Scientific Advisors
Dave Jones
Managing Partner of Sail Ventures
Henry T. Harbin, MD
Former Chair and CEO of Magellan
Jerry Vaccaro, MD
President of APS Healthcare, former President of United
Behavioral/PacifiCare
-------------------------
Alan F. Schatzberg, MD
Chairman Department of Psychiatry, Stanford Medical School
Maurizio Fava, MD
Associate Chief of Psychiatry for Clinical Research, Massachusetts
General and Professor Psychiatry Harvard Medical School
Steve Suffin, MD
Head Pathologist Science and Technology, Quest Diagnostics, CNSO
founder
Max Schneider, MD
Former Chair of ASAM, CSAM, NCADD

17
I haven’t told you the real story. The real
story is best told by doctors and patients.
Len Brandt
CEO
CNS Response, Inc.
714.545.3225
lbrandt@cnsresponse.com
Many people – patients, doctors and payers
thank you for your attention.
Horace Hertz
CFO
CNS Response, Inc
714.545.2954
hhertz@cnsresponse.com