UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
WASHINGTON, D.C. 20549
FORM
For the fiscal year ended
OR
For the transition period from to
Commission File Number:
(Exact name of Registrant as specified in its charter)
2834 |
||
(State or Other Jurisdiction of |
(Primary Standard Industrial |
(I.R.S. Employer |
Incorporation or Organization) |
Classification Code Number) |
Identification No.) |
(Address of principal executive offices, including zip code)
(
(Registrant’s telephone number, including area code)
Securities registered pursuant to Section 12(b) of the Act:
Title of each class |
Trading Symbol(s) |
Name of each exchange on which registered |
None |
|
|
Securities Registered Pursuant to Section 12(g) of the Act:
Title of class |
Indicate by check mark if the registrant is a well‑known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes ☐
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act. Yes ☐
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days.
Indicate by check mark whether the registrant has submitted electronically every Interactive Data File required to be submitted pursuant to Rule 405 of Regulation S‑T (§ 232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit such files).
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non‑accelerated filer, a smaller reporting company, or emerging growth company. See the definitions of “large accelerated filer,” “accelerated filer,” “smaller reporting company” and “emerging growth company” in Rule 12b‑2 of the Exchange Act:
Large accelerated filer |
☐ |
|
|
Accelerated filer |
☐ |
☒ |
|
|
Smaller reporting company |
||
Emerging growth company |
|
|
|
|
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ☐
Indicate by check mark whether the registrant has filed a report on and attestation to its management’s assessment of the effectiveness of its internal control over financial reporting under Section 404(b) of the Sarbanes-Oxley Act (15 U.S.C. 7262(b)) by the registered public accounting firm that prepared or issued its audit report.
If securities are registered pursuant to Section 12(b) of the Act, indicate by check mark whether the financial statements of the registrant included in the filing reflect the correction of an error to previously issued financial statements. ☐
Indicate by check mark whether any of those error corrections are restatements that required a recovery analysis of incentive-based compensation received by any of the registrant's executive officers during the relevant recovery period pursuant to §240.10D-1(b). ☐
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Act). Yes ☐ No
The aggregate market value of shares of common stock held by non‑affiliates of the registrant as of June 30, 2022, the last business day of the registrant’s most recently completed second fiscal quarter, was $
There were
1
TABLE OF CONTENTS
ITEM |
|
|
PAGE |
|
3 |
||
|
|
|
|
|
4 |
||
|
|
||
ITEM 1. |
6 |
||
ITEM 1A. |
22 |
||
ITEM 1B. |
44 |
||
ITEM 2. |
44 |
||
ITEM 3. |
45 |
||
ITEM 4. |
45 |
||
|
|
||
ITEM 5. |
46 |
||
ITEM 6. |
46 |
||
ITEM 7. |
MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS |
47 |
|
ITEM 7A. |
55 |
||
ITEM 8. |
55 |
||
ITEM 9. |
CHANGES IN AND DISAGREEMENTS WITH ACCOUNTANTS ON ACCOUNTING AND FINANCIAL DISCLOSURE |
55 |
|
ITEM 9A. |
55 |
||
ITEM 9B. |
56 |
||
ITEM 9C. |
DISCLOSURE REGARDING FOREIGN JURISDICTIONS THAT PREVENT INSPECTIONS. |
56 |
|
|
|
||
ITEM 10. |
57 |
||
ITEM 11. |
60 |
||
ITEM 12. |
SECURITY OWNERSHIP OF CERTAIN BENEFICIAL OWNERS AND MANAGEMENT AND RELATED STOCKHOLDER MATTERS |
63 |
|
ITEM 13. |
CERTAIN RELATIONSHIPS AND RELATED TRANSACTIONS, AND DIRECTOR INDEPENDENCE |
64 |
|
ITEM 14. |
65 |
||
|
|
||
ITEM 15. |
67 |
||
74 |
|||
2
CAUTIONARY STATEMENT REGARDING FORWARD‑LOOKING STATEMENTS
This Annual Report contains some statements that are not purely historical and that are considered “forward‑looking statements” within the meaning of Section 27A of the Securities Act of 1933, as amended, which we refer to as the Securities Act, and Section 21E of the Securities Exchange Act of 1934, as amended, which we refer to as the Exchange Act. Such forward‑looking statements express our management’s expectations, beliefs, and intentions regarding the future. The words “anticipates,” “believes,” “continue,” “could,” “estimates,” “expects,” “intends,” “may,” “might,” “plans,” “possible,” “potential,” “predicts,” “projects,” “seeks,” “should,” “will,” “would” and similar expressions and variations, or comparable terminology, or the negatives of any of the foregoing, may identify forward‑looking statements, but the absence of these words does not mean that a statement is not forward‑looking.
The forward‑looking statements contained in this Annual Report are based on current expectations and beliefs concerning future developments that are difficult to predict. We cannot guarantee future performance, or that future developments affecting our company will be those currently anticipated. These forward‑looking statements involve risks, uncertainties (some of which are beyond our control) or assumptions that may cause actual results or performance to be materially different from those expressed or implied by these forward‑looking statements, including the factors referenced in this Annual Report under the sections entitled “Business,” “Risk Factors” and “Management’s Discussion and Analysis of Financial Condition and Results of Operations.”
All forward‑looking statements attributable to us are expressly qualified in their entirety by these risks and uncertainties, and you should not place undue reliance on any forward‑looking statement. We undertake no obligation to update or revise any forward‑looking statement, except as may be required under applicable securities laws.
3
RISK FACTOR SUMMARY
Following is a summary of certain material risks and uncertainties facing our business. This summary is not a complete discussion of the risk and uncertainties affecting us. A more complete discussion of these and other risks and uncertainties is set forth under “Risk Factors” in Part I, Item 1A of this Annual Report. Additional risks not presently known to us or that we presently deem immaterial may also affect us. If any of these risks occur, our business, financial condition or results of operations could be materially and adversely affected.
Risks Related to Our Business
We have operated at a loss and may continue to operate at a loss for the foreseeable future.
We are dependent on financing to sustain our operations, and there is substantial doubt regarding our ability to continue as a going concern.
We are dependent on the commercial success of our only approved product, Endari®.
We face intense competition from companies with greater resources than us, and if our competitors are successful in marketing or developing alternative treatments, our commercial opportunities may be reduced or eliminated.
The majority of Endari® sales are to a few customers and loss of a customer could adversely affect our results of operations.
The market exclusivity for Endari® for sickle cell disease (“SCD”) in the U.S. is limited and Endari® will have no market exclusivity in the Kuwait, Qatar or the United Arab Emirates, where Endari® is approved for marketing, the Kingdom of Saudi Arabia or other countries in the Middle East North Africa ("MENA") region where applications for marketing approval are pending, which lack of exclusivity could adversely affect the commercial success of Endari® even if approved for marketing.
A variety of risks associated with marketing Endari® internationally could hurt our business.
We expect to rely on third parties to conduct future clinical trials of our product candidates and those third parties may not perform satisfactorily, including failing to meet deadlines for the conduct of such trials.
The use of any of our product candidates in clinical trials and in the market may expose us to liability claims.
We will need to increase the size and complexity of our organization in the future, and we may experience difficulties in managing our growth and executing our growth strategy.
Historical material weaknesses in our internal controls over financial reporting have not been fully remediated.
Risks Related to Our Intellectual Property
We may not be able to obtain and enforce intellectual property rights that cover our commercial activities or are sufficient to prevent third parties from competing against us.
Risks Related to Regulatory Oversight of Our Business and Compliance with Law
Endari® is subject to ongoing and continued regulatory review, compliance with which may result in significant expense and limit our ability to commercialize Endari®.
We may not be able to receive eventual regulatory approval of PGLG treatment for diverticulosis or other indications, which would adversely affect our future prospects.
The development process to obtain U.S. Food and Drug Administration ("FDA") approval for new drug therapies is very costly and time consuming and if we cannot complete our clinical trials in a cost-effective manner, our operations may be adversely affected.
4
If we fail to comply with federal and state healthcare laws, including fraud and abuse and health information privacy and security laws, we could face substantial penalties and our business, results of operations, financial condition and prospects could be adversely affected.
Orphan Drug designation for Endari® will expire in mid-2024, and we may not be able to maintain Orphan Drug marketing exclusivity for Endari® or any of our product candidates.
Risks Related to Our Investment in EJ Holdings, Inc.
EJ Holdings has no revenues and is dependent on us to fund its business and operations, and there is no assurance that we can continue to provide needed funding or that EJ Holdings will be able to continue its activities.
If EJ Holdings fails to reactivate its plant and obtain customers, it may not be able to sell its plant and property and we may lose our investment.
EJ Holdings is subject to risks inherent in a new business and may not be successful.
Risks Related to Our Securities
Trading on the OTC Markets is volatile and sporadic, which could depress the market price of our common stock and make it difficult for our investors and stockholders to buy or resell our common stock.
Stockholders may experience future dilution from future equity offerings.
Our common stock is not traded on a national securities exchange, which may adversely affect our ability to raise needed financing.
Our stockholders have authorized our board of directors to effect a reverse stock split of our common stock, but if the board does so it may not result in the intended benefits.
5
PART I
ITEM 1. BUSINESS
In this Annual Report, the terms, “we,” “us,” “our” or the “Company” refer to Emmaus Life Sciences, Inc., and its subsidiaries.
Overview
Endari®
We are a commercial-stage biopharmaceutical company engaged in the discovery, development, marketing and sale of innovative treatments and therapies, primarily for rare and orphan diseases. Our lead product, Endari® (prescription grade L-glutamine oral powder) is approved by the U.S. Food and Drug Administration, or FDA, to reduce the acute complications of sickle cell disease (“SCD”) in adult and pediatric patients five years of age and older. Endari® has received Orphan Drug designation from the FDA, which designation affords marketing exclusivity for Endari® in the U.S. for a seven-year period expiring in July 2024.
Endari® is marketed and sold in the U.S. by our internal commercial sales team. Endari® is reimbursable by the Centers for Medicare and Medicaid Services, and every state provides coverage for Endari® for outpatient prescriptions to all eligible Medicaid enrollees within their state Medicaid programs. Endari® is also reimbursable by many commercial payors. We have agreements in place with the nation’s leading distributors, as well as physician group purchasing organizations and pharmacy benefits managers, making Endari® available at selected retail and specialty pharmacies nationwide.
SCD is a rare, debilitating and lifelong hereditary blood disorder that affects approximately 100,000 patients in the U.S. and up to 25 million patients worldwide, the majority of which are of African descent. Approximately one in every 365 African-American children are born with SCD. The FDA’s approval of Endari® was based upon the results of a 48-week randomized, double-blind, placebo-controlled, multi-center Phase 3 clinical trial evaluating the effects of Endari®, as compared to placebo in 230 adults and children with SCD. The results demonstrated that Endari® reduced the frequency of sickle cell crises by 25% and hospitalizations by 33%. Additional findings included a 41% decrease in cumulative hospital days and greater than 60% fewer incidents of acute chest syndrome in patients treated with Endari®. The FDA has acknowledged that the clinical benefit of Endari® was observed irrespective of hydroxyurea use, which supports the use of Endari® as a monotherapy or in combination with hydroxyurea as safe and effective treatment options for patients with SCD.
The safety of Endari® was based upon data from 298 patients, 187 treated with Endari® and 111 patients treated with placebo in Phase 2 and Phase 3 studies. Endari®’s safety profile was similar to the placebo and Endari® was well-tolerated in pediatric and adult patients alike. The most common adverse reactions, occurring in more than 10% of patients treated with Endari®, were constipation, nausea, headache, abdominal pain, cough, pain in extremity, back pain, and chest pain (non-cardiac).
6
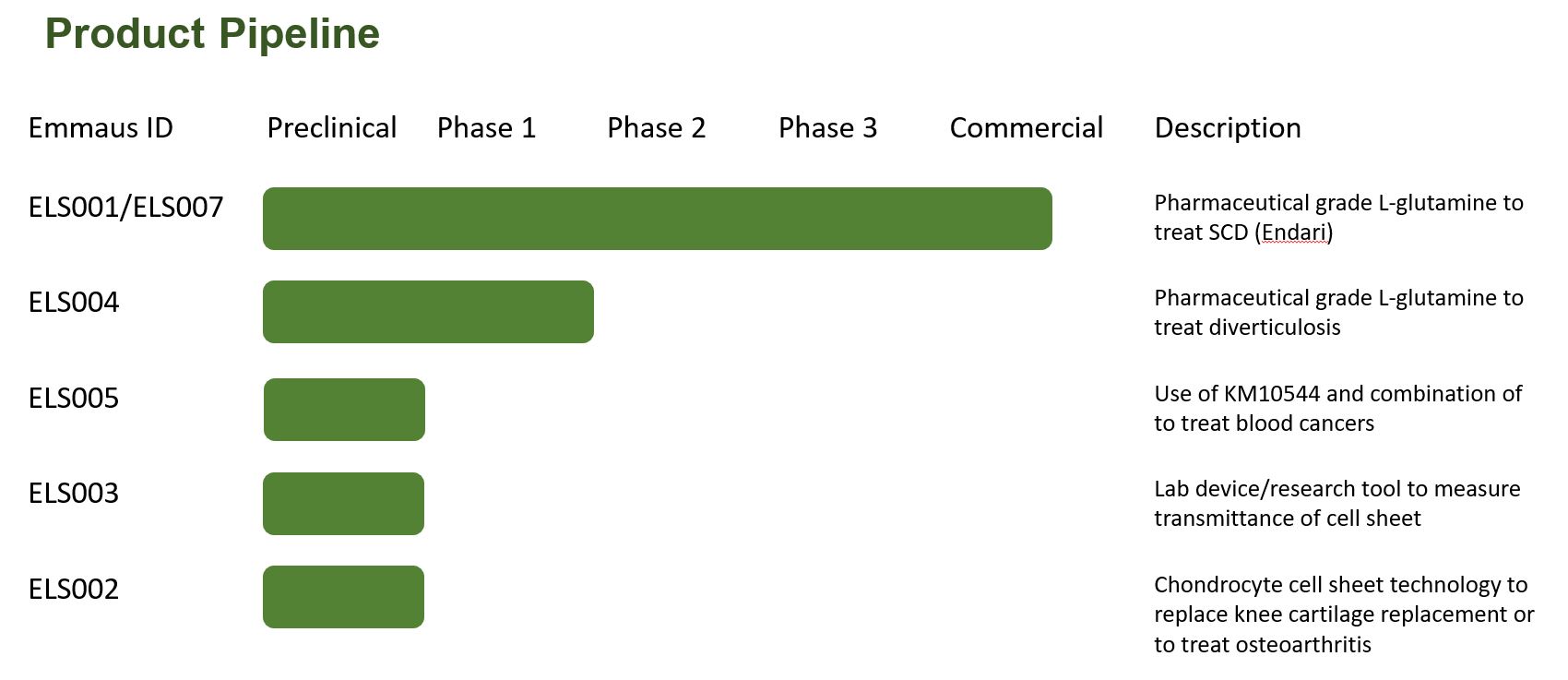
Product Pipeline
The following table summarizes our product pipeline:
Diverticulosis
On July 4, 2018, the FDA acknowledged receipt of our investigational new drug application, or IND, for the treatment of diverticulosis using the same prescription grade L-glutamine oral powder (“PGLG”) used for Endari® (L-glutamine oral powder). We subsequently received a “Study May Proceed” letter from the FDA. In April 2019, we commenced a Pilot/Phase 1 study of the safety and efficacy of PGLG oral powder in diverticulosis. The study evaluated the change in the number and size of colonic diverticula and assess safety in a total of 10 evaluable patients at multiple study sites.
The last patient visit for the pilot study was in November 2021. The data obtained after 12 months of treatment with L-glutamine was inconclusive, so we initiated a sub-study in June 2021, through an amendment to the original IND protocol. The sub-study standardized data collection and recording using video capture to support the accurate assessment of any changes in the sigmoid colon, the most frequent site for diverticulosis, as well as diverticulitis, a more severe manifestation of diverticulosis. The objective of the sub-study was to provide additional safety and efficacy data to support further clinical development. The sub-study colonoscopy procedures were assessed by a central medical monitor in addition to the treating investigator. For the sub-study, at least five patients were administered oral L-glutamine 15g BID over six months. The data from the sub-study, which was completed in July 2022, also was inconclusive. There were no safety concerns reported in either the Pilot/Phase 1 or the sub-study.
We may determine to undertake further investigation of the effectiveness of PGLG in patients with a history of diverticulitis but have no current plan to do so.
Oncology Project
On October 7, 2021, we entered into a License Agreement with Kainos Medicine, Inc., a South Korean corporation (“Kainos”), under which Kainos has granted us an exclusive license in the territory encompassing the U.S., the U.K. and the EU to patent rights, know-how and other intellectual property relating to Kainos’s novel IRAK4 inhibitor, referred to as KM10544, for the treatment of cancers, including leukemia, lymphoma, and solid tumor cancers. Based upon the positive pre-clinical results, we intend to conduct further testing in vivo to evaluate KM10544’s toxicity and efficacy against targeted cancers, including acute myeloid leukemia and Waldenstrom Macroglobulinemia.
Chondrocyte Cell Sheet Technology
We have developed chondrocyte and osteoblast “cell sheets” using human mesenchymal stem cells and are conducting pre-clinical studies to assess the potential of the cell sheets to articular cartilage injury, osteoarthritis and other
7
cartilage-related conditions and bone diseases such as osteoarthritis, nonunion and Paget’s disease. A cell sheet is a composite of cells grown and harvested in an intact sheet, rather than as individual cells, and can be used for tissue transplantation or to engineer complex multilayer cell sheets composed of different types of cells. Our cell sheets offer several potential advantages over existing treatment options, including reduced chemical toxins and xeno-products needed during cell sheet generation, easier and more convenient cell coverage of the injured tissue (transplantation on the damaged area), and allogeneic (i.e., use of stem cells from one individual in another individual) transplantation.
Cultured Autologous Oral Mucosal Epithelial Cell Sheets (CAOMECS)
An Emmaus-led team at The Lundquist Institute, or TLI, an independent non-profit biomedical research organization academically affiliated with the David Geffen School of Medicine at University of California, at Los Angeles that works in partnership with Harbor-UCLA Medical Center, is conducting pre-clinical studies of Cultured Autologous Oral Mucosal Epithelial Cell Sheet, or CAOMECS technology. This study is sponsored by Emmaus, and the lead CAOMECS program is for the treatment of corneal diseases.
Device Measuring Cell Sheets Transparency
We also have developed a device for measuring the maturity of biological cell cultures for harvesting of cell sheets, as well as the number cells and the cell sheet transparency, in one or more cell sheets of the biological cell cultures. This semi-automatic device is a potentially essential tool for quality control in the growing field of cell sheet translational medicine. The potential application of this device includes assessment of the transparency of donor’s cornea before transplantation. Currently, there is no objective method to assess the timing for cell sheet harvesting and to assess the donor’s cornea transparency for corneal transplantation. We have filed a patent application in the U.S. for this technology and are in the process of improving the device. We may seek a potential partner to develop or commercialize the device.
Summary of Pipelines Products
The development of our potential anti-cancer treatments, cell sheet technologies including chondrocyte cell sheets for treating cartilage and bone related conditions and CAOMECS for treating corneal and other diseases are in the early stages.
Recent Highlights
In December 2022, we received an Endari Marketing Authorization from the Pharmaceutical and Herbal Medicines Registration and Control Administration (Drug and Foods Control) of the Kuwait Ministry of Health.
In November 2022, we received an Endari Marketing Authorization from the Registration Committee for Pharmaceutical Companies & their Products of the Qatar Ministry of Public Health.
In April 2022, we announced the launch of innovative full-service Telehealth Solution with its strategic partners, including Asembia LLC and UpScript IP Holdings, LLC.
In March 2022, we received approval for marketing of Endari to treat SCD from the United Arab Emirates (U.A.E.) Ministry of Health.
Sickle Cell Disease—Market Overview
Sickle cell disease (“SCD”) is a genetic blood disorder that affects 20 million - 25 million people worldwide and occurs with increasing frequency among those whose ancestors are from regions including sub-Saharan Africa, South America, the Caribbean, Central America, the Middle East, India and Mediterranean regions such as Turkey, Greece and Italy. The U.S. Centers for Disease Control and Prevention estimates that there are as many as 100,000 people with SCD in the United States, and we estimate there are approximately 80,000 SCD sufferers in the EU. We estimate that there are over 100,000 SCD patients that could potentially be treated in the Persian Gulf States, as well as patients in other countries that comprise the Middle East and North Africa (“MENA”) region.
SCD is characterized by the production of an altered form of hemoglobin which polymerizes and becomes fibrous, causing the red blood cells of patients with SCD to become sickle‑shaped, inflexible and adhesive rather than round, smooth and flexible. These changes also lead to increased oxidant stress and much damage to the membrane of red blood cells. It also causes increased adhesiveness of red blood cells. The complications associated with SCD occur when these inflexible and
8
sticky cells block, or occlude, small blood vessels, which can then cause severe and chronic pain throughout the body due to insufficient oxygen being delivered to tissue, or ischemia, and inflammation. According to an article in Annals of Internal Medicine, “In the Clinic: Sickle Cell Disease” by M.H. Steinberg (September 2011), which we refer to as the Steinberg Article, this leads to long‑term organ damage, diminished exercise tolerance, increased risk of stroke and infection and decreased lifespan.
Sickle cell crisis, a broad term covering a range of disorders, is one of the most devastating complications of SCD. Types of sickle cell crisis include:
According to the Steinberg Article referred to above, acute chest syndrome affects more than half of all patients with SCD and is a common reason for hospitalization. Other symptoms and complications of SCD include swelling of the hands and feet, infections, pneumonia, vision loss, leg ulcers, gall stones and stroke.
A crisis is characterized by excruciating musculoskeletal pain, visceral pain and pain in other locations. These crises occur periodically throughout the life of a person with SCD. In adults, the acute pain typically persists for five or ten days or longer, followed by a dull, aching pain generally ending only after several weeks and sometimes persisting between crises. According to the Steinberg Article, the frequency of sickle cell crises varies within patients with SCD from rare occurrences to occurrences several times a month. The frequency of crises tends to increase late in the second decade of life and to decrease after the fourth decade.
Treatment of sickle cell crises is burdensome and expensive for patients and payors, as it encompasses costs for hospitalization, urgent care and emergency room visits and prescription pain medication. Endari® enhances nicotinamide adenine dinucleotide (“NAD”) synthesis to reduce excessive oxidative stress in sickle red blood cells, which is the cause of much of the damage leading to characteristic symptoms of SCD. We believe that Endari®, when taken daily, will decrease the incidence of sickle cell crisis by restoring the flexibility, fluidity and function of red blood cells in patients with SCD. We believe that regular use of Endari® also will reduce the number of costly hospitalizations of patients with SCD, as well as unexpected urgent care and emergency room visits.
Limitations of the Current Standard of Care
Prior to the approval of Endari®, the only other FDA approved pharmaceutical targeting sickle cell crisis was hydroxyurea, which is available in both generic and branded formulations. Hydroxyurea, a drug originally developed as an anticancer chemotherapeutic agent, has been approved as a once‑daily oral treatment for reducing the frequency of sickle cell crisis and the need for blood transfusions in adult patients with recurrent moderate to severe sickle cell crisis. In December 2017, the FDA granted Addmedica a regular approval for hydroxyurea (Siklos) to reduce the frequency of painful crises and the need for blood transfusions in pediatric patients two years of age and older with sickle cell anemia with recurrent moderate to severe painful crises. While hydroxyurea has been shown to reduce the frequency of sickle cell crisis in some patient groups, it is not suitable for many patients due to significant toxicities and side effects. In particular, hydroxyurea can cause a severe decrease in the number of blood cells in a patient’s bone marrow, which may increase the risk that the patient will develop a serious infection or bleeding, or that the patient will develop certain cancers. Another potential treatment option for SCD, bone marrow transplant, is limited in its use due to the lack of availability of matched donors and the risk of serious complications, including graft versus host disease, infection and potentially death, as well as by its high cost.
9
Two new treatments for sickle cell disease were approved by the FDA at the end of 2019. Crizanlizumab, marketed under the brand name of Adakveo® by Novartis AG, is a humanized monoclonal antibody that binds to P-selectin. It is approved by the FDA to reduce the frequency of vaso-occlusive crises in adults and pediatric patients aged 16 years and older with SCD. It is administered intravenously in two loading doses two weeks apart and every four weeks thereafter. Voxelotor, marketed under the brand name of Oxbryta™ by Pfizer Inc., is an HbS polymerization inhibitor that reversibly binds to hemoglobin to stabilize the oxygenated hemoglobin state, thus shifting the oxyhemoglobin dissociation curve. Oxbryta™ is approved by the FDA for the treatment of SCD in adults and pediatric patients 12 years of age and older. In December 2021, the FDA granted accelerated approval for Oxbryta to treat SCD in pediatric patients aged 4 to less than 12 years.
Upon onset of sickle cell crisis, the current standard of care is focused on pain management, often with prescription narcotics or non-prescription oral medications taken at home. If the pain is not relieved, or if it progresses, patients may seek medical attention in a clinic or emergency department. Pain that is not controlled in these settings may require hospitalization for more potent pain medications, typically opioids administered intravenously. The patient must stay in the hospital to receive these intravenous pain medications until the sickle cell crisis resolves and the pain subsides. Other supportive measures during hospitalization may include hydration, supplemental oxygen and treatment of any concurrent infections or other conditions.
According to Hematology in Clinical Practice, by Robert S. Hillman et. al. (5th ed. 2011), sickle cell crisis, once it has started, almost always results in tissue damage at the affected site in the body, increasing the importance of preventative measures. While pain medications can be effective in managing pain during sickle cell crisis, they do not affect or resolve the underlying vascular occlusion, tissue ischemia or potential tissue damage. Additionally, opioid narcotics that are generally prescribed to treat pain can also lead to tissue or organ damage and resulting complications and morbidities, prolonged hospital stays and associated continuation of pain and suffering. Given the duration and frequency of sickle cell crises, addiction to these opioid narcotics is also a significant concern.
Endari®, Our Solution for SCD
We believe Endari® may provide a safe and effective means for reducing the frequency of sickle cell crises in patients with SCD and the need for costly hospital stays or treatment with highly addictive pain medications such as opioid narcotics. Published academic research has identified L-glutamine as a precursor to NAD, one of the major molecules that regulate and prevent oxidative damage in red blood cells. Several published studies have demonstrated that sickle red blood cells have a significantly increased rate of transport of L-glutamine, which appears to be driven by the cells’ synthesis of NAD to protect against oxidative damage and thereby leading to further improvement in their regulation of oxidative stress. In turn this makes sickle red blood cells less adhesive to cells of the interior wall of blood vessels, which suggests that there is decreased chance of blockage of blood vessels, especially small ones. In summary, improved regulation of oxidative stress appears to lead to less obstruction or blockage of small blood vessels, thereby alleviating a major cause of the pain and other problems associated with SCD.
In December 2013, we completed a Phase 3 prospective, randomized, double blind, placebo controlled, parallel group multicenter clinical trial to measure, over a 48-week time frame, as its primary outcome, the reduction in the number of occurrences of sickle cell crises experienced by patients in the trial. All participants other than those who received placebo, including children, received up to 30 grams of Endari® daily, dissolved in liquid, split between morning and evening; the same dosage as our Phase 2 clinical trial completed in 2009. Patients were randomized to the study treatment using a 2:1 ratio of Endari® to placebo. The randomization was stratified by investigational site and hydroxyurea usage.
The clinical trial evaluated the efficacy and safety of Endari® in 230 patients (5 to 58 years of age) with sickle cell anemia or sickle β°-thalassemia who had 2 or more painful crises within 12 months prior to enrollment. Eligible patients stabilized on hydroxyurea for at least 3 months continued their therapy throughout the study. The trial excluded patients who had received blood products within 3 weeks, had renal insufficiency or uncontrolled liver disease, or were pregnant (or planning pregnancy) or lactating. Study patients received Endari® or placebo for a treatment duration of 48 weeks followed by 3 weeks of tapering.
10
Efficacy was demonstrated by a reduction in the number of sickle cell crises through Week 48 and prior to the start of tapering among patients that received Endari® compared to patients who received placebo. A sickle cell crisis was defined as a visit to an emergency room/medical facility for sickle cell disease-related pain which was treated with a parenterally administered narcotic or parenterally administered ketorolac. In addition, the occurrence of acute chest syndrome, priapism, and splenic sequestration were considered sickle cell crises. Treatment with Endari® also resulted in fewer hospitalizations due to sickle cell pain at Week 48, fewer cumulative days in hospital, longer time until first sickle cell crisis and a lower incidence of acute chest syndrome.
Table 1. Results from the Endari® Clinical Trial in Sickle Cell Disease
|
Endari |
Placebo |
Event |
(n = 152) |
(n = 78) |
Median number of sickle cell crises (min, max)1 |
3 (0, 15) |
4 (0, 15) |
Median number of hospitalizations for sickle cell pain (min, max)1 |
2 (0, 14) |
3 (0, 13) |
Median cumulative days hospitalized (min, max)1, |
6.5 (0, 94) |
11 (0, 187) |
Median time (days) to first sickle cell crisis (95% CI) 1,2 |
84 (62, 109) |
54 (31, 73) |
Patients with occurrences of acute chest syndrome (%)1 |
13 (8.6%) |
18 (23.1%) |
1. Measured through 48 weeks of treatment.
2. Hazard Ratio=0.69 (95% CI=0.52, 0.93), estimated based on unstratified Cox’s proportional model. Median time and 95% CI were estimated based on the Kaplan Meier method.
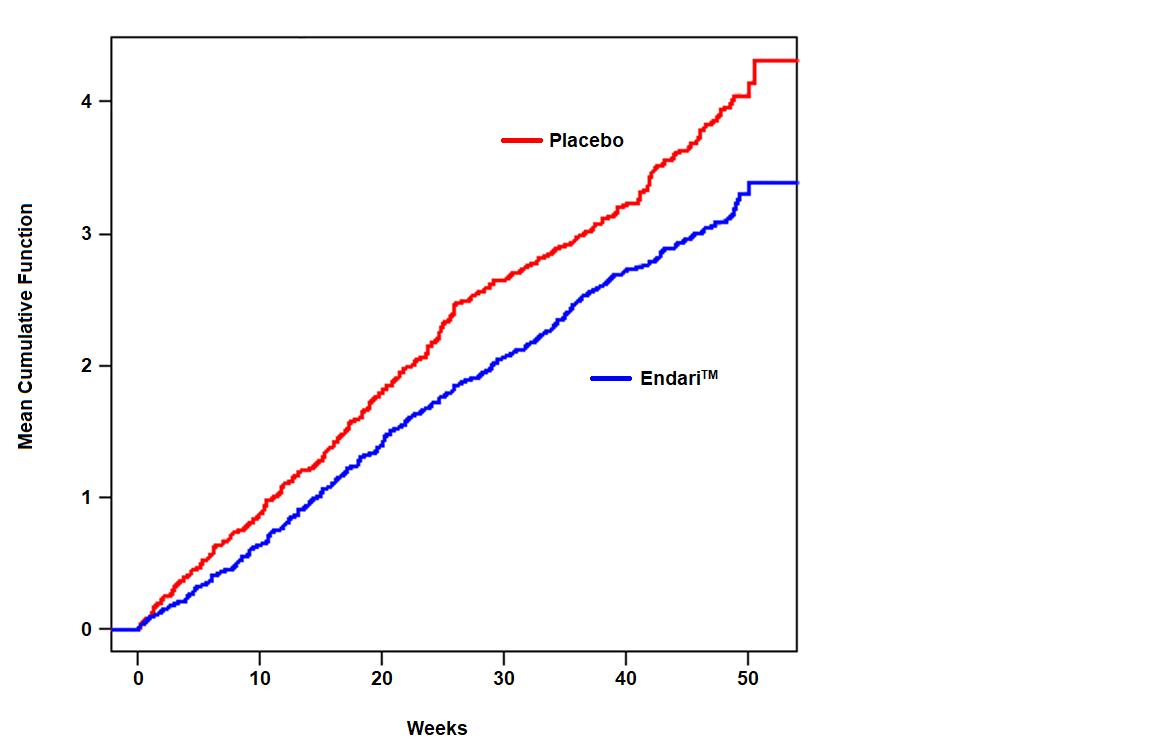
The recurrent crisis event time analysis (Figure 1) yielded an intensity rate ratio (IRR) value of 0.75 with 95% CI= (0.62, 0.90) and (0.55, 1.01) based on unstratified models using the Andersen-Gill and Lin, Wei, Yang and Ying methods, respectively in favor of Endari®, suggesting that over the entire 48- week period, the average cumulative crisis count was reduced by 25% from the Endari® group over the placebo group.
Figure 1. Recurrent Event Time for Sickle Cell Crises by Treatment Group
Endari® was studied in 2 placebo-controlled clinical trials (a phase 3 study, n=230 and a phase 2 study, n=70). In these trials, patients with sickle cell anemia or sickle β0-thalassemia were randomized to receive Endari® (n=187) or placebo (n=111) orally twice daily for 48 weeks followed by 3 weeks of tapering. Both studies included pediatric and adult patients (5-58 years of age) and 54% were female.
11
Treatment discontinuation due to adverse reactions was reported in 2.7% (n=5) of patients receiving Endari®. These adverse reactions included one case each of hypersplenism, abdominal pain, dyspepsia, burning sensation, and hot flash.
Commercialization and Distribution
United States
Our in-house commercial team encompasses marketing, market access, patient support, and distribution support personnel. The sales team consists of sales representatives and sales management personnel. We have a Commercial Patient Assistance Program (C- PAP) to provide financial assistance to eligible patients who are unable to afford their monthly co-payments for Endari®. We also maintain the Endari® Patient Support Program to provide eligible patients access to Endari® where appropriate.
Our sales and marketing efforts focus on the following groups: pediatric and adult hematologists who treat SCD patients, Community Based Organizations, or CBOs, government payors, insurance companies, and pharmacy benefit managers. SCD patients are primarily treated at specialized clinics located in children’s hospitals, university hospitals and community-based out-patient locations. The current focus of our sales team is as follows:
We have contracted with AmerisourceBergen Specialty Group (ASD Healthcare LLC), AmerisourceBergen Corporation companies, McKesson Plasma and Biologics LLC, a McKesson Corporation company, Cardinal Health 108, LLC, a Cardinal Health Inc. company, and CVS Caremark, L.L.C., a CVS Health Corporation company, to distribute Endari® to selected pharmacies and hospitals. AmerisourceBergen Corporation, McKesson Corporation Cardinal Health, Inc and Caremark are the four largest specialty distributors of prescription drugs in the U.S.
Our two largest distributors, ASD Healthcare LLC and McKesson Plasma and Biologics LLC, each account for more than 25% of net revenue for the year ended December 31, 2022. On a combined basis, these distributors accounted for approximately 79% of net revenue in 2022.
Outside the United States
In May 2019, we announced that the European Medicines Agency’s Committee for Medicinal Products for Human Use, or CHMP, adopted a negative opinion regarding our application for marketing authorization, or MAA, for our prescription grade L-glutamine oral powder, to be known as Xyndari™ in the European Union, or EU based upon the CHMP’s position that our main clinical study did not conclusively support Xyndari™'s efficacy, although no safety concerns were raised. In light of the CHMP’s opinion, we withdrew our MAA. We are considering whether to pursue possible alternative regulatory pathways in an effort to afford SCD patients in EU countries access Xyndari™.
Post-Brexit, we assessed our overall submission package to determine strategies for scientific advice from the United Kingdom, or U.K., Medicines and Healthcare Products Regulatory Agency in preparation for a possible submission of a MAA for Xyndari™. We expect to provide an update of our assessment in the second half of 2023.
We have entered into exclusive distribution agreements with strategic partners to register, commercialize and distribute Endari® in the Gulf Cooperation Council countries, or GCC, and other countries throughout the MENA region in collaboration with our branch office in Dubai. Marketing authorizations have been approved in GCC countries, the United Arab Emirates (March 2022), Qatar (November 2022), and Kuwait (December 2022) and are pending in Kingdom of Saudi Arabia and Bahrain.
We are party to an exclusive early access agreement pursuant to which our strategic partner distributes Endari® on an early access basis in France, the Netherlands and the U.K. We also are in talks with potential strategic partners in other
12
countries to establish similar early access programs while we consider seeking marketing authorization in one of more of such countries.
We also may seek future collaborations with other pharmaceutical or biotechnology companies and identify potential licensees and other international opportunities to commercialize Endari®, if approved by foreign regulatory authorities.
Diverticulosis
Diverticulosis, or the presence of colonic diverticula (i.e., pouches in the colon wall), is very common in industrialized nations, with its prevalence increasing with age. An estimated 40% of 60 year-olds and 70% of 80 year-olds have diverticulosis. Of these individuals, 10% to 25% are expected to develop diverticulitis, or the advancement of peri diverticular inflammation and infection, resulting in abdominal pain, nausea, vomiting, constipation, diarrhea, fever, and leukocytosis.
The pathogenesis of diverticulosis is believed to result from structural abnormalities of the colonic wall, disordered motility and low fiber diets. The relationships between glutamine and intestinal physiology have been extensively studied in ulcerative colitis and Crohn’s disease, short bowel syndrome and as a nutritional therapy for critical illnesses. Overall, glutamine elicits the following mechanisms of action within intestinal cells: promotion of enterocyte proliferation, regulation of tight junction proteins; suppression of pro-inflammatory signaling pathways; suppression of intestinal cell apoptosis and cellular stress; and microbiome regulation. Glutamine also helps to maintain intestinal tissue integrity through various signaling pathways.
See the discussion above of our Pilot/Phase 1 study and substudy of the safety and efficacy of prescription grade L-glutamine oral powder in diverticulosis.
We are party to a distributor agreement with Telcon RF Pharmaceutical, Inc., or Telcon pursuant to which we granted Telcon exclusive rights to our PGLG oral powder for the treatment of diverticulosis in South Korea, Japan and China. The agreement contemplates that Telcon will be responsible at its expense for obtaining marketing authorization assuming FDA approval is obtained and for all other commercial activities in the territories. In exchange for the exclusive rights, Telcon paid us a $10 million upfront fee, which is refundable in the event of termination of the distributor agreement for failure to obtain FDA approval. See the “Raw Materials and Manufacturing,” below, for more information on our arrangements with Telcon.
Oncology Project
On October 6th, 2021, we licensed a small molecule (KM10544) targeting IRAK4 signaling pathway to treat leukemia and lymphomas. Leukemia is a cancer of blood-forming tissue causing high variation of its manifestation and therefore requiring many different treatment options. While there has been increase in survival rate by seven years from treatment of younger patient population (i.e., less than 60 years) since 1970, the survival rate has increased only one year for patients older than 60 years. Waldenstrom macroglobulinemia (WM) is a rare blood cancer that accounts for 1% to 2% of all hematological malignancies. In the U.S., around 1000 to 5000 new cases are detected each year. Many of the WM patients are asymptomatic making it difficult to detect and treat WM in its early stages.
We are conducting pre-clinical studies to assess KM10544’s efficacy in two cancer cell lines, acute myeloid leukemia and Waldenstrom macroglobulinemia. In in vitro studies, KM10544 suppressed the proliferation and induced apoptosis (cell death) in both cancer cell lines with minimal toxic effects in healthy human cell lines, including human dermal fibroblasts and human adipose stromal cells. We plan to undertake further in vivo testing to evaluate its toxicity (maximal dose and side effects) and to determine how KM-10544 cans affect (tumor elimination, delay of growth) against acute myeloid leukemia and WM.
Cultured Autologous Oral Mucosal Epithelial Cell Sheets (CAOMECS)
A team at The Lundquist Institute (TLI), a non-profit biomedical research organization academically affiliated with the David Geffen School of Medicine at University of California, at Los Angeles that works in partnership with Harbor-UCLA Medical Center, sponsored by Emmaus, is conducting a pre-clinical study developing Cultured Autologous Oral Mucosal Epithelial Cell Sheet, or CAOMECS, technology to reconstruct the ocular surface of patients with corneal blindness. CAOMECS is a cell sheet composite of cells grown and harvested in an intact sheet, rather than as individual cells. These cell sheets can be used for tissue transplantation or to engineer complex multilayer cell sheets composed of different types of cells. In the pre-clinical study, these rabbits cell sheets were engineered using specialized media not containing any animal
13
products. In this perspective, KaFa medium was developed to eliminate the use of murine feeder cells, fetal bovine serum ((FBS) thus TSE/BSE free), cholera toxin, and animal-origin produced growth factors and hormones, thus reducing the risk of transmitting inherent organism specific carrier diseases. The composition of the xeno-free medium includes reagents components that are FDA-approved with Drug Master File numbers. The development and successful formulation of KaFa medium will make engineering cell sheets a safe graft for human use in clinical applications without the current risks inherent to use of non-human reagents. The effectiveness of our newly developed KaFa medium has been demonstrated during pre-clinical studies performed using oral mucosal epithelial cells isolated from a small biopsy of rabbit buccal tissue. Using a donor's oral mucosal epithelial cells, we are working toward being able to grow and harvest a human cell sheet for autologous grafting onto the cornea of the affected eye to repair the damaged cornea. The development of CAOMECS for treating corneal and other diseases, including limbal stem cell deficiency, has been successful in at least one animal study.
Thrombospondin-1 induction and VEGF reduction, by proteasome inhibitor, could to alleviate corneal neovascularization
The anti-angiogenic thrombospondin-1 (TSP-1) has been shown to be a natural inhibitor of neovascularization and the pro-angiogenic vascular endothelial growth factor (VEGF) has been shown to promote neovascularization. The simultaneous increase in TSP-1 and decrease in VEGF expressions might alleviate corneal neovascularization contributing to enhancing corneal transparency and visual acuity.
Chondrocyte Cell Sheet Technology
We have developed human cartilage and bone multilayer cell sheets using human adult mesenchymal stem cells and are conducting preclinical studies to assess the restorative properties of these cell sheets. Cartilage cell sheets have the potential to treat diseases such as articular cartilage injury and osteoarthritis. Bone cell sheets are potentially useful in treating diseases such as osteoarthritis, nonunion and Paget’s disease. This cell sheet technology offers several potential advantages over the existing treatment options. The harvesting does not require any special treatment, such as the use of enzymes which could be harmful to the treated cells and patients. Current treatments options involve the injection of individual cells to the damaged area, which requires identification of precise injection location and multiple injections due to rapid cell death. In addition, injection of single cells could have a long-term effect with an ectopic settlement of cells leading to impairment of organ function. In contrast, cell sheet technology allows wider coverage of needed cells to the damaged cartilage and higher cell survival due to the cell sheet structure.
Unlike existing cell therapies, our cell sheets can be produced from mesenchymal stem cells from donors for use on other patients, referred to as allogeneic transplantation. Due to the mesenchymal stem cells unique immune properties the risk of immune rejection is lower compared to organ’s transplantation. These advantages should eventually lead to lower-cost and more efficient production of the cell sheets.
This technology is supported by the PCT Patent International Application No. PCT/US2022/047381 filed on October 21, 2022, entitled “Engineering of Stratified Cell Sheets Using Human Mesenchymal Stem Cells”.
Device Measuring Cell Sheets Transparency
We have developed a semi-automatic device for quality control in the cell-sheet manufacturing process. This device measures the maturation of the biological cell culture over-time to estimate the harvesting time of the cell sheets, number of cells present in one or more cell sheets of the biological cell culture, and transparency of biological cell culture. The application of this device extends to ophthalmology to assess the transparency of donor’s cornea before transplantation. Currently there is no objective method to assess the donor’ cornea to understand readiness or compatibility.
This technology is supported by the PCT Patent International Application No. PCT/US2022/011267, entitled “System and Method of Evaluating Cell Culture,” filed on January 5, 2022.
Research and Development
We incurred $1.7 million and $4.1 million of research and development expenses in 2022 and 2021, respectively. The decrease primarily related to the acquisition of KM10544 from Kainos in 2021 and a decrease in expenses in 2022 relating to a pharmacokinetic characteristic and safety study for Endari® in the U.S. and a clinical study in Europe.
Raw Materials and Manufacturing
The active pharmaceutical ingredient in Endari® is prescription grade L‑glutamine (“PGLG”) oral powder, which differs from non‑prescription grade L‑glutamine widely available as a nutritional supplement. Endari® is differentiated from
14
ordinary L-glutamine by several factors, including the presence of a Drug Master File, oversight of purity and manufacturing at FDA inspected facilities, and stringent stability tested packaging. There are limited suppliers of PGLG worldwide, and we currently obtain substantially all our PGLG, directly or indirectly, from Ajinomoto Health and Nutrition North America, Inc. (“Ajinomoto”), a subsidiary of Ajinomoto North American Holdings, Inc.
Ajinomoto provided PGLG to us free of charge for our clinical trials of Endari®, including our Phase 3 trial. In return, we undertook to purchase from Ajinomoto substantially all our commercial needs for PGLG, subject to certain exceptions; however, we have no long-term supply agreement with Ajinomoto.
On June 16, 2017, we entered into an API supply agreement with Telcon (formerly, Telcon, Inc.), a South Korea-based company, pursuant to which Telcon paid us approximately ₩36.0 billion KRW (approximately $31.8 million) in consideration of the right to supply 25% of our requirements for bulk containers of PGLG for a 15-year term. The amount was recorded as a deferred trade discount. The API supply agreement provides for target annual revenue of more than $5,000,000 and annual “profit” (i.e., sales margin) to Telcon of at least $2,500,000 commencing in 2018. On July 12, 2017, we entered into a raw material supply agreement with Telcon which revised certain terms of the API supply agreement, which we refer to as the “revised API agreement.” The revised API agreement is effective for a term of five years and will renew automatically for 10 successive one-year renewal periods, except as either party may determine. In the revised API agreement, we have agreed to purchase a cumulative total of $47.0 million of PGLG over the term of the agreement. In September 2018, we entered into an agreement with Ajinomoto and Telcon to facilitate Telcon’s purchase of PGLG from Ajinomoto for resale to us under the revised API agreement. The PGLG raw material purchased from Telcon is recorded in inventory at net realizable value and the excess purchase price is recorded against deferred trade discount.
Our obligations under the agreements with Telcon are secured by a pledge of a convertible bond of Telcon purchased by us under a Convertible Bond Purchase Agreement dated September 28, 2020. See Note 11 and Note 14 of the Notes to Consolidated Financial Statements in this Annual Report for more information regarding our obligations under the various agreements with Telcon.
In December 2019, EJ Holdings, Inc., or EJ Holdings a Japanese corporation which is 40% owned by us, purchased from Kyowa Hakko Bio Co. Ltd., or Kyowa, a subsidiary of Kyowa Hakko Kirin Co., Ltd., Kyowa’s phased-out facility in Ube, Japan, for the manufacture of L-glutamine and other amino acids. EJ Holdings is engaged in phasing in the plant, including obtaining FDA and other regulatory approvals for the manufacture of PGLG in accordance with current Good Manufacturing Practices (“cGMP”). Once the plant is active, we expect to enter into a long-term agreement with EJ Holdings for the supply of PGLG. We currently anticipate that test production will commence later in 2023. EJ Holdings has had no revenues since its inception, has depended on loans from us to acquire the Ube plant and fund its operations and will continue to be dependent on loans from us or other financing unless and until its plant is activated and it can secure customers, including us, for its products. As of December 31, 2022, we had loaned EJ Holdings a total of $25.0 million. In addition to any further loans from us, EJ Holdings is expected to require substantial financing in order bring the Ube plant online. EJ Holdings has no commitments or understandings regarding any additional financing. Under the asset purchase agreement pursuant to which EJ Holdings purchased the Ube plant, Kyowa has the right to repurchase the plant at the purchase price of $10.4 million plus certain taxes paid by EJ Holdings if the plant does not become operational within a reasonable period (not to exceed five years).
In May 2020 we entered into a memorandum of understanding and agreement, or MOU, with Japan Industrial Partners, Inc., or JIP, which owns 60% of the capital stock of EJ Holdings, to memorialize the parties’ intentions with respect to the business and operations of the Ube plant and ownership of EJ Holdings. The MOU contemplates, among other things, that we will continue to be the principal source of funding for EJ Holdings’ ownership and operation of the plant and that, subject to certain conditions, to the extent we provide additional funding our ownership interest in EJ Holdings is expected to increase accordingly and that the composition of EJ Holdings’ board of directors and control of EJ Holdings would be modified consistent with the parties’ relative ownership interests. The MOU also contemplates that the Ube plant will eventually supply us with the plant’s output of amino acids and that the operation of the plant will be principally for our benefit and, accordingly, that major decisions affecting EJ Holdings and the Ube plant will be made by EJ Holdings’ board of directors in consultation with us. At present, JIP owns 60% of EJ Holdings and is entitled to designate a majority of EJ Holdings’ board of directors, its Chief Executive Officer, and outside auditors, and as such, controls the management, business and operations of EJ Holdings.
Endari® and any other commercial products we develop must be manufactured and packaged by facilities that meet FDA requirements for cGMP. We believe that Ajinomoto and Packaging Coordinators, Inc., or PCI, of Rockville, Illinois, which packages Endari®, meet FDA cGMP. Previous compliance with cGMP; however, does not guarantee future
15
compliance. We have no long-term agreement with PCI. We may seek to enter into long-term supply agreements in the future and to establish one or more arrangements with alternative suppliers, including EJ Holdings.
Competition
The biopharmaceutical industry is highly competitive and subject to rapid and significant technological change. We face potential competition from both large and small pharmaceutical and biotechnology companies, academic institutions, governmental agencies (such as the National Institutes of Health) and public and private research institutions. Many of our competitors and potential competitors have far greater financial resources and expertise in research and development, manufacturing, preclinical testing, conducting clinical trials, obtaining regulatory approvals, marketing and selling approved products. Historically, for example, we have had insufficient financial resources to engage in meaningful advertising or marketing of Endari®. Smaller or early-stage companies may also prove to be significant competitors, particularly through collaborative arrangements with large and established companies.
Any product candidates that we successfully develop and commercialize will compete with existing therapies and new therapies that may become available in the future. The key competitive factors affecting the success of each of our product candidates, if approved, are likely to be their safety, efficacy, convenience, price, the level of proprietary and generic competition, and the availability of coverage and reimbursement from government and other third‑party payors. Our Endari® sales may suffer or our commercial opportunity could be reduced or eliminated if our competitors develop and commercialize products that are safer or more effective, have fewer or less severe side effects, or are more convenient or less expensive than any products that we may develop. Our competitors may also obtain FDA or other regulatory approval for their product candidates more rapidly than we may be able to do so for any existing or new product candidates of ours, which could result in their establishing a strong market position before we are able to enter the market.
Sickle Cell Disease
Endari® is approved as a therapy to reduce the acute complications of SCD in adult and pediatric patients 5 years of age and older. The other drugs which are indicated to treat sickle cell disease are hydroxyurea (marketed as DROXIA or Hydrea by Bristol-Myers Squibb Company and available in generic form), which is approved to reduce the frequency of painful crises and need for blood transfusions in patients with sickle cell anemia for the treatment of adults with SCD; Voxelotor (marketed as Oxbryta™ by Global Blood Therapeutics, Inc.) tablets for the treatment of SCD in adults and children 4 years of age and older; and crizanlizumab (marketed as Adakveo® by Novartis International AG) intravenous infusion approved to reduce the frequency of VOCs in adult and pediatric patients ages 16 years and older with SCD. Several companies are also developing product candidates for chronic treatment in SCD, and several other companies are in clinical trials to investigate new treatments for SCD.
Endari® also faces potential competition from one-time therapies for treating patients with severe SCD, including LentiGlobin BB305, which is being developed by bluebird bio, Inc. to treat SCD by inserting a functional human beta-globin gene into a patient’s hematopoietic stem cells, or HSCs, ex vivo and then transplanting the modified HSCs into the patient’s bloodstream. Bluebird has indicated its plans to pursue an accelerated development and approval pathway for its gene therapy product in SCD. Others are seeking to develop one-time therapies such as hematopoietic stem cell transplantation, gene therapy and gene editing, including gene editing using CRISPR. Attempts to develop a cure for SCD through gene therapy are in the early stages, but if these attempts were to succeed and receive regulatory approval, it could adversely affect the market for Endari®.
We are also aware of efforts to develop cures for SCD through approaches such as bone marrow treatments. Although bone marrow transplant is currently available for SCD patients, its use is limited by the lack of availability of matched donors and by the risk of serious complications, including graft versus host disease and infection.
Endari® also competes with non-prescription grade L-glutamine, which is widely available as a dietary supplement at substantially lower prices than Endari®. Dietary supplements may be marketed without FDA approval, are generally not reimbursed by payors and are not subject to the rigorous quality control standards required by regulatory authorities for prescription drug products. Also, unlike prescription drugs, manufacturers of dietary supplements may not make claims that the supplements will cure, mitigate, treat or prevent disease, and we are not aware of any reports in peer-reviewed literature regarding the effectiveness of non-prescription grade L-glutamine supplements in treating SCD in controlled clinical trials.
Diverticulosis
There is no currently FDA-approved treatment for diverticulosis.
16
Oncology Treatment
IRAK-4 is a popular targeted pathway of inflammatory diseases, including cancers. In our pre-clinical studies, Kainos’s novel IRAK-4 inhibitor, referred to as KM10544, has shown promising signs of efficacy against FLT-3 positive leukemia cell lines and other hematological malignancy cell lines such as Waldenstrom Macroglobulinemia cell line.
KM10544 technology is supported by the PCT Patent International Application No. PCT/US2022/023632, entitled “Compositions and Methods For Treating Cancer”, filed on April, 6 2022.
Chondrocyte Cell Sheet Technology
Currently, no cell therapy to treat damaged bone has been approved by the FDA, using mesenchymal stem cells. Only 1 cell therapy was approved by the FDA to treat cartilage (Tradename: MACI), but this approved therapy requires the use of porcine collagen membrane, the use of animal product (serum) and it is an autologous transplantation of patient’s cartilage. However, this cell therapy can’t be used for patient’s carrying genetic mutation or for patients with no cartilage. According to available data from clinicaltrial.gov, there is only one clinical trial of the efficacy of cartilage cell sheets, “Safety and Efficacy Study of Cells Sheet-Autologous Chondrocyte Implantation to Treat Articular Cartilage Defects (CS-ACI)” (Xijing Hospital, Xi'an Shi, China; Tangdu Hospital, Xi’an Shi, China; Xi’An Honghui Hospital, Xi'an Shi, China) (ClinicalTrials.gov Identifier: NCT01694823).
The development of cell sheets using mesenchymal stem cells (e.g adipose stromal cells), may lead to new treatments of patients. In addition, the cell sheets were engineered using animal-free culture media and have the potential translational application for allogeneic transplantation. Our cell sheet therapy also makes possible to layer different types of cell sheets by harvesting the cell sheet without the use of harmful enzymes (trypsin or dispase) that may damage the cell‑based therapy and potentially to construct in vitro stratified tissue equivalents by alternately layering different types of harvested cell sheets to provide regenerated tissue architectures, resembling human tissues. For example, cartilage cell sheets can be layered on the top of a bone cell sheet before transplantation if the patient’s health condition requires it. This technique holds promise for the study of cell‑cell communications and angiogenesis in reconstructed, three‑dimensional environments, as well as for tissues engineering with complex, multicellular architectures, and drug-screening.
Cultured Autologous Oral Mucosal Epithelial Cell Sheets (CAOMECS)
Currently, the treatment of limbal stem cell deficiency (“LSCD”) varies based on the severity of the LSCD. Treatment may include the use of non-invasive procedures such as autologous serum drops, therapeutic scleral lens and corneal scraping to more invasive surgical procedures such as grafting limbal stem cells biopsied from the fellow eye or from an allogenic donor eye. The use of patient’s limbal stem cells for autologous transplantation increases the risk of damaging the healthy eye, probably leading to a bilateral limbal stem cell deficiency. Transplantation with cells other than from the patient’s own tissue can cause serious complications, including rejection of transplanted tissue or donor’s cells carry genetic mutation causing LSCD (e.g., p63). Using CAOMECS technology lessens these risks, if LSCD is not due to a genetic mutation. Specifically, the use of CAOMECS decreases the risk of graft rejection, and mainly permits treatment of bilateral LSCD patients and allows engineered corneal epithelial cell sheets reconstruct the ocular surface of LSCD patients.
The development of CAOMECS technology to treat LSCD is in the early stages. We are not aware of any FDA approved treatments using CAOMECS for LSCD.
Research institutions outside the United States (e.g., The Centre Hospitalier National d’Ophtalmologie des Quinze Vingts lin Paris, France; Royan Institute Teheran in the Islamic Republic of Iran and Hospital San Raffaele in Milan, Italy; UCLA, Los Angeles, USA; Chang Gung Memorial Hospital, Taipei, Taiwan) are developing the transplantation of corneal cells from patients’ healthy eyes to reverse LSCD. However, results from these clinical trials were not published yet. This approach only allows unilateral LSCD patients to be treated and risks damage to the patients’ one healthy corneas.
CAOMECS is a promising alternative for the treatment of LSCD. For example, the Chang Gung Memorial Hospital (Taiwan) (ClinicalTrials.gov Identifier: NCT03943797) is conducting a phase 1, The Hospices Civils de Lyon (France) is conducting a phase 2 (ClinicalTrials.gov Identifier: NCT03949881), and the He Eye Hospital China (ClinicalTrials.gov Identifier: NCT03015779), the Adisak Wongkajornsilp, Siriraj Hospital in Thailand (ClinicalTrials.gov Identifier: NCT02415218) has finished a phase 2 clinical trials using the OMEC. While many research institutions as are conducting such trials, we are not aware of published results of these studies on clinicaltrials.gov.
Our OMEC-based regenerative medicine technology eliminates risks associated with donor-dependent transplantation as it is an autologous technology developed by using the patient own cells. OMEC-based regenerative
17
medicine technology has shown promising results in pilot studies (animal serum dependent) done by other groups in Japan and Europe. Our innovative technology utilizes cell sheet therapy was developed in xeno-free cell culture conditions (free of animal based-products) that allows harvesting cell sheets with intact extracellular matrix (fibronectin, laminin, collagen type IV), reducing the inherent risks of suturing during transplantation.
Government Regulation
The FDA has granted Endari Orphan Drug designation and the EC has granted our PGLG Orphan Medicinal designation for the treatment of SCD.
Orphan Drug Designation. The FDA has authority under the U.S. Orphan Drug Act to grant Orphan Drug designation to a drug or biological product intended to treat a rare disease or condition. This law defines a rare disease or condition generally as one that affects fewer than 200,000 individuals in the United States, or more than 200,000 individuals in the United States and for which there is no reasonable expectation that the cost of the development and distribution of the orphan product in the United States will be recovered from sales of the product. Being granted Orphan Drug designation provides tax benefits to mitigate expenses of developing the orphan product. More importantly, Orphan Drug designation provides seven years of market exclusivity if the product receives the first FDA approval for the disease or condition for which it was granted such designation and the indication for which approval is granted matches the indication for which Orphan Drug designation was granted. During the seven-year exclusivity period, Orphan Drug exclusivity precludes FDA approval of a marketing application for the same active ingredient for the same indication. Orphan Drug exclusivity is limited and will not preclude the FDA from approving the same active ingredient for the same indication if the same product is shown to be clinically superior to the product previously granted exclusivity. In addition, a product that is the same as the orphan product may receive approval for a different indication (whether orphan or not) during the exclusivity period of the orphan product. Also, Orphan Drug market exclusivity will not bar a different product such as Pfizer Inc., Therapeutics, Inc.’s Oxbryta to treat the same orphan disease or condition from obtaining its own Orphan Drug designation and Orphan Drug exclusivity.
The Orphan Drug designation for Endari will expire July 7, 2024, after which date Endari may face competition from generic PGLC products. In the meantime, we may pursue improvements and reformulations of Endari to seek preserve our intellectual property rights in Endari following the expiration of its Orphan Drug designation.
Orphan Medicinal status in the EU has similar benefits, including a ten-year marketing exclusivity period following marketing authorization in the EU.
There is no designation available in the U.A.E. or other countries in the MENA region similar to Orphan Drug or Orphan Medicinal designations, so we will not be entitled to marketing exclusivity in the region for Endari® in Kuwait, Qatar, the U.A.E. or other countries in the region where we may obtain marketing authorization.
505(b)(2) Applications. Under Section 505(b)(2) of the Federal Food, Drug, and Cosmetic Act (“FD&C Act”), a person may submit an NDA for which one or more of the clinical studies relied upon by the applicant for approval were not conducted by or for the applicant and for which the applicant does not have a right of reference or use from the person by or for whom the clinical studies were conducted. Instead, a 505(b)(2) applicant may rely on published literature containing the specific information (e.g., clinical trials, animal studies) necessary to obtain approval of the application. The applicant may also rely on the FDA’s finding of safety and/or effectiveness of a drug previously approved by the FDA when the applicant does not own or otherwise have the right to access the data in that previously approved application. The 505(b)(2) pathway to marketing authorization thus allows an applicant to submit a NDA without having to conduct its own studies to obtain data that are already documented in published reports or previously submitted NDAs. In addition to relying on safety data from the Phase 2 and 3 studies of Endari®, we intend to take advantage of the 505(b)(2) pathway to the extent published literature will further support any NDA for PGLG.
Regulation by United States and foreign governmental authorities is a significant factor in the development, manufacture and expected marketing of our product candidates and in our ongoing research and development activities. The nature and extent to which such regulation will apply to us will vary depending on the nature of the product candidates we seek to develop.
Human therapeutic products, such as drugs, biologics and cell-based therapies, are subject to rigorous preclinical and clinical testing and other preapproval requirements of the FDA and similar regulatory authorities in other countries. Various federal and state statutes and regulations govern and influence pre- and post-approval requirements related to research, testing, manufacturing, labeling, packaging, storage, distribution and record keeping of such products to ensure the safety and effectiveness for their intended uses. The process of obtaining marketing approval and ensuring post approval
18
compliance with the FD&C Act for drugs and biologics (and applicable provisions of the Public Health Service Act for biologics), and the regulations promulgated thereunder, and other applicable federal and state statutes and regulations, requires substantial time and financial resources. Any failure by us or our collaborators to obtain, or any delay in obtaining, marketing approval could adversely affect the marketing of any of our product candidates, our ability to receive product revenues, and our liquidity and capital resources.
The manufacture of these products is subject to cGMP regulations. The FDA inspects manufacturing facilities for compliance with cGMP regulations before deciding whether to approve a product candidate for marketing.
The steps required by the FDA before a new product, such as a drug, biologic or cell-based therapy, may be marketed in the United States include:
In addition to obtaining FDA approval for each product candidate before we can market it as a product, the manufacturing establishment from which we obtain it must be registered and is subject to periodic FDA post approval inspections to ensure continued compliance with cGMP requirements. If, as a result of these inspections, the FDA determines that any equipment, facilities, laboratories, procedures or processes do not comply with applicable FDA regulations and the conditions of the product approval, the FDA may seek civil, criminal, or administrative sanctions and/or remedies against us, including the suspension of the manufacturing operations, recalls, the withdrawal of approval and debarment. Manufacturers must expend substantial time, money and effort in the area of production, quality assurance and quality control to ensure compliance with these standards.
Preclinical testing includes laboratory evaluation of the safety of a product candidate and characterization of its formulation. Preclinical testing is subject to Good Laboratory Practice (“GLP”) regulations. Preclinical testing results are submitted to the FDA as a part of an IND which must become effective prior to commencement of clinical trials. Clinical trials are typically conducted in three sequential phases following submission of an IND. In Phase 1, the product candidate under investigation (and therefore often called an investigational product) is initially administered to a small group of humans, either patients or healthy volunteers, primarily to test for safety (e.g., to identify any adverse effects), dosage tolerance, absorption, distribution, metabolism, excretion and clinical pharmacology, and, if possible, to gain early evidence of effectiveness. In Phase 2, a slightly larger sample of patients who have the condition or disease for which the investigational product is being studied receive the investigational product to assess the effectiveness of the investigational product, to determine dose tolerance and the optimal dose range, and to gather additional information relating to safety and potential adverse effects. If the data show the investigational product may be effective and has an acceptable safety profile in the targeted patient population, Phase 3 studies, also referred to as pivotal studies or enabling studies, are initiated to further establish clinical safety and provide substantial evidence of the effectiveness of the investigational product in a broader sample of the general patient population, to determine the overall risk benefit ratio of the investigational product, and provide an adequate basis for physician and patient labeling. During all clinical studies, Good Clinical Practice (“GCP”) standards and applicable human subject protection requirements must be followed. The results of the research and product development, manufacturing, preclinical studies, clinical studies, and related information are submitted in a NDA to the FDA.
19
The process of completing clinical testing and obtaining FDA approval for a new therapeutic product, such as a drug, biologic or cell-based product, is likely to take years and require the expenditure of substantial resources. If a NDA is submitted, there can be no assurance that the FDA will file, review, and approve it. Even after initial FDA approval has been obtained, post market studies could be required to provide additional data on safety or effectiveness. Additional pivotal studies would be required to support adding other indications to the labeling. Also, the FDA will require post market reporting and could require specific surveillance or risk mitigation programs to monitor for known and unknown side effects of the product. Results of post marketing programs could limit or expand the continued marketing of the product. Further, if there are any modifications to the product, including changes in indication, manufacturing process, labeling, or the location of the manufacturing facility, a NDA supplement would generally be required to be submitted to the FDA prior to or corresponding with that change, or for minor changes in the periodic safety update report that must be submitted annually to the FDA.
The rate of completion of any clinical trial depends upon, among other factors, sufficient patient enrollment and retention. Patient enrollment is a function of many factors, including the size of the patient population, the nature of the trial, the number of clinical sites, the availability of alternative therapies, the proximity of patients to clinical sites, and the eligibility and exclusion criteria for the trial. Delays in planned patient enrollment might result in increased costs and delays. Patient retention could be affected by patient noncompliance, adverse events, or any change in circumstances making the patient no longer eligible to remain in the trial.
Failure to adhere to regulatory requirements for the protection of human subjects, to ensure the integrity of data, other IND requirements, and GCP standards in conducting clinical trials could cause the FDA to place a “clinical hold” on one or more studies of a product candidate, which would stop the studies and delay or preclude further data collection necessary for product approval. Noncompliance with GCP standards would also have a negative impact on the FDA’s evaluation of a NDA. If at any time the FDA finds that a serious question regarding data integrity has been raised due to the appearance of a wrongful act, such as fraud, bribery or gross negligence, the FDA may invoke its Application Integrity Policy (“AIP”) under which it could immediately suspend review of any pending NDA or refuse to accept the submission of a NDA as filed, require the sponsor to validate data, require additional clinical studies, disapprove a pending NDA or withdraw approval of marketed products, as well as require corrective and preventive action to ensure data integrity in future submissions. Significant noncompliance with IND regulations could result in the FDA not only refusing to accept a NDA as filed but could also result in enforcement actions, including civil and administrative actions, civil money penalties, criminal prosecution, criminal fines and debarment. Whether or not FDA approval has been obtained, approval of a product by regulatory authorities in foreign countries must be obtained prior to the commencement of marketing the product in those countries.
The requirements governing the conduct of clinical trials and product approvals vary widely from country to country, and the time required for approval might be longer or shorter than that required for FDA approval. Although there are some procedures for unified filings for some European countries, in general, each country at this time has its own procedures and requirements.
In most cases, if the FDA has not approved a product candidate for sale in the United States, the unapproved product may be exported to any country in the world for clinical trial or sale if it meets U.S. export requirements and has marketing authorization in any listed country without submitting an export request to the FDA or receiving FDA approval to export the product, as long as the product meets the regulatory requirements of the country to which the product is being exported. Listed countries include each member nation in the European Union or the European Economic Area, Canada, Australia, New Zealand, Japan, Israel, Switzerland and South Africa. If an unapproved product is not approved in one of the listed countries, the unapproved product may be exported directly to an unlisted country if the product meets the requirements of the regulatory authority of that country, and the FDA determines that the foreign country has statutory or regulatory requirements similar or equivalent to the United States.
In addition to the regulatory framework for product approvals, we and our collaborative partners must comply with federal, state and local laws and regulations regarding occupational safety, laboratory practices, the use, handling and disposition of radioactive materials, environmental protection and hazardous substance control, and other local, state, federal and foreign regulation. All facilities and manufacturing processes used by third parties to produce our product candidates for clinical use in the United States and our products for commercialization must be in compliance with cGMP requirements and are subject to periodic regulatory inspections. The failure of third-party manufacturers to comply with applicable regulations could extend, delay or cause the termination of clinical trials conducted for our product candidates or the withdrawal of our products from the market. The impact of government regulation upon us cannot be predicted and could be material and adverse. We cannot accurately predict the extent of government regulation that might result from future legislation or administrative action.
20
Patents, Proprietary Rights and Know‑How
Our success will depend in part on our ability to obtain patents and otherwise preserve the intellectual property rights relating to the design, operation, sale and distribution of our products. We intend to seek patents on our products when we deem it commercially appropriate. The process of seeking patent protection can be lengthy and expensive, and there can be no assurance that patents will be issued for currently pending or future applications or that our existing patents or any new patents issued will be of sufficient scope or strength or provide meaningful protection or any commercial advantage to us. We may be subject to, or may initiate, litigation or patent office interference proceedings, which may require significant financial and management resources. The failure to obtain necessary licenses or other rights or the advent of litigation arising out of any such intellectual property claims could have a material adverse effect on our operations.
We have relied to date on a combination of patent licenses, trademark rights, trade secret protection, distribution agreements, manufacturing agreements, manufacturing capability and other unpatented proprietary information to protect our intellectual property rights. While we do not currently own any issued patents directed to the treatment of sickle cell anemia, we do own patent applications in that area, as well as issued patents and patent applications directed to the treatment of diverticulosis, diabetes and hypertriglyceridemia. We have Orphan Drug market exclusivity for the treatment of sickle cell anemia with Endari® in the United States through July 7, 2024 and, if approved in the EU, for ten years from the approval date. We may seek to pursue improvements and reformulations of Endari® to preserve our intellectual property rights in Endari following the expiration of its Orphan Drug designation.
We also rely on employee agreements to protect the proprietary nature of our products. We require that our officers and key employees enter into confidentiality agreements that require these officers and employees to assign to us the rights to any inventions developed by them during their employment with us. All the confidentiality agreements include non-solicitation provisions that remain effective during the course of employment and for periods following termination of employment.
Patents
We have issued patents related to compositions including PGLG and methods involving administration of PGLG for the treatment of diverticulosis in the United States, Europe, Japan, Australia, India, Mexico, China, Indonesia, Korea and Russia. Associated patent applications are currently pending in the United States, the EU, Brazil, Korea and Russia.
Patents directed to compositions for decreasing HbA1C levels in individuals who are shown to have average blood sugar levels in the diabetic range have issued in Japan, Indonesia and the Philippines. Associated applications are currently pending in the United States, Europe, Brazil, India, China, the Philippines, and Japan.
We have issued patents directed to the treatment of hypertriglyceridemia in Japan and the Philippines. A corresponding European patent application has been granted and is currently the subject of an Opposition proceeding. Associated applications are pending in the United States, Brazil, India, China, and the Philippines.
A patent application directed to the treatment of sickle cell using a multi-component composition is pending in the United States and Europe. An international application directed to the same invention has been filed under the Patent Cooperation Treaty.
We have a pending international (PCT) patent application directed to the treatment of cancers with KM10544, alone or in combination with a Bruton Tyrosine Kinase (BTK) inhibitor or a Poly (ADP-ribose) polymerase (PARP) inhibitor. The cancers being treated may have a MyD88 mutation (e.g., the L265P missense mutation) and can include hematologic cancers, such as Waldenstrom Macroglobulemia (WM), Acute Myeloid Leukemia (AML), and diffuse large B-cell lymphoma (DLBCL), and solid tumors such as rectal cancer, pancreatic cancer, and small cell lung cancer. The application is expected to enter into national stages by June 2024 and has a projected expiration date in 2042.
We have a pending PCT patent application directed to devices and methods for measuring the thickness of cell sheets. The technology is important for the preparation and use of stem cell-derived cells sheets, such as corneas and cell sheets. This non-invasive approach can determine the time progression of cell sheet growth, the maturity of the cell sheet, and the number of cells per cell sheet before harvesting and transplantation. The application is expected to enter into national stages by July 2023 and has a projected expiration date in 2042.
We have a pending PCT patent application directed to the preparation and use of cell sheets. The prepared cell sheets can be used for the treatment of cartilage-related conditions such as cartilage injury and osteoarthritis, and bone
21
diseases such as nonunion bone diseases and Paget’s disease. The cell sheets can be formed of a multilayer of cells grown and harvested in an intact cell sheet that can be transplanted as a patch on the injured area. The application is expected to enter into national stages by April 2024 and has a projected expiration date in 2042.
License Agreements
On October 7, 2021, we entered into a License Agreement with Kainos, under which Kainos granted us an exclusive license in the territory encompassing the U.S., the U.K. and the EU to patent rights, know-how and other intellectual property relating to Kainos’s IRAK4 inhibitor, referred to as KM10544, for the treatment of cancers, including leukemia, lymphoma and solid tumor cancers. In consideration of the license, we paid Kainos a six-figure upfront fee in cash and agreed to make future cash payments upon the achievement of specified milestones totaling in the mid-eight figures, a single-digit percentage royalty based on net sales of the licensed products and a similar percentage of any sublicensing consideration. The License Agreement will continue on a licensed product-by-licensed product and country-by-country basis until the last to expire valid claim of any licensed patent in such country.
Trademarks
We hold U.S. trademark registrations for “Emmaus Medical” and “Endari” and a trademark registration for “Xyndari™” (as Endari® will be marketed if approved) in the EU. This Annual Report also contains trademarks, service marks, trade names and copyrights of other companies, which are the property of their respective owners. Solely for convenience, these trademarks, service marks, trade names and copyrights may appear without the® or TM symbols, but such references are not intended to indicate that we or the other owners do not assert, to the fullest extent under applicable law, our rights, or the rights of any licensor to the same.
Employees
As of December 31, 2022, we had 55 employees, 54 of whom were full time. We have not experienced any work stoppages and we consider our relations with our employees to be good.
Corporate Information
We were incorporated in Delaware on March 20, 1987 under the name Age Research, Inc. Prior to January 16, 2007, our company (then called Strativation, Inc.) existed as a “shell company” with nominal assets and whose sole business was to identify, evaluate and investigate various companies to acquire or with which to merge. On January 16, 2007, we entered into an Agreement and Plan of Merger with CNS Response, Inc., and CNS Merger Corporation, our wholly owned subsidiary, pursuant to which CNS Merger Corporation merged with and into CNS Response, Inc., which survived the merger. On March 7, 2007, we changed our corporate name to CNS Response, Inc. On November 2, 2015, we changed our corporate name to MYnd Analytics, Inc. On July 17, 2019, we completed our merger transaction with EMI Holding, Inc., formerly known as Emmaus Life Sciences, Inc. (“EMI”), with EMI surviving as our wholly owned subsidiary. On July 17, 2019, immediately following the merger, we changed our name to “Emmaus Life Sciences, Inc.”
Our principal executive offices and corporate offices are located at 21250 Hawthorne Boulevard, Suite 800, Torrance, California, and our telephone number at that address is (310) 214‑0065. We maintain an Internet website at the following address: www.emmausmedical.com. The information on our website is not incorporated by reference in this Annual Report or in any other filings we make with the Securities and Exchange Commission (“SEC”).
ITEM 1A. RISK FACTORS
Risks Related to Our Business
We have operated at a loss and may continue to operate at a loss for the foreseeable future.
We realized comprehensive loss of $13.0 million for the year ended December 31, 2022, compared to comprehensive loss of $17.3 million for the year ended December 31, 2021, and have historically operated at a loss due to substantial expenditures related to commercialization of Endari®, loan funding to EJ Holdings, Inc., to support its activities as described below, pursuit of marketing authorization of Endari outside the U.S., interest on our outstanding indebtedness, general and administrative expenses and research and development of our product candidates. While we anticipate increased net revenues as we expand our commercialization of Endari® in the U.S. through telehealth and other initiatives, as well as in the MENA region, there is no assurance that we will be able to increase our Endari® sales or attain sustainable profitability
22
or that we will have sufficient capital resources to fund our operations until we are able to generate sufficient cash flow from operations.
We are dependent on financing to sustain our operations, and there is substantial doubt regarding our ability to continue as a going concern.
Unless and until we become profitable, we will continue to depend upon proceeds from related-party loans, third-party loans, sales of our debt or equity securities (including the exercise of options and warrants) or other financing arrangements, or possible payments from potential strategic partners and licensees to generate funds needed to finance our business and operations. As of December 31, 2022, we had cash and cash equivalents of $2.0 million and a working capital deficit of $48.0 million. Depending upon our future results of operations and other factors, we will need additional financing to fund our business and operations, including providing funding to EJ Holdings, Inc. as described below under “Risks Related to Our Investment in EJ Holdings, Inc.,” and will continue to be dependent on future financing until such time, if ever, as we can generate sufficient revenues to become profitable. We have no current understanding or arrangement to obtain any additional related-party or third-party loans or other financing. Accordingly, we may not be able to obtain future financing on favorable terms, or at all. If we are unable to obtain needed future financing, we may have to curtail some of our business activities or modify our business plans and may be unable to repay our outstanding indebtedness or continue providing funding to EJ Holdings, Inc.
In light of the foregoing, there is substantial doubt regarding our ability to continue as a going concern and the report of our independent public accounting firm on our financial statements as of and for the year ended December 31, 2022 contains a going concern explanatory paragraph.
We are dependent on the commercial success of our only approved product, Endari®.
Our ability to become profitable will depend upon the commercial success of Endari®. In addition to the risks discussed elsewhere in this section, our ability to generate future revenues from Endari® sales will depend on a number of factors, including, but not limited to:
Because of the numerous risks and uncertainties associated with our commercialization efforts, we are unable to predict the extent of revenues we will generate from Endari® sales or the timing for when or the extent to which we will become and continue to be profitable, if ever. Even if we do achieve increased net revenues from Endari® sales and become profitable, we may not be able to sustain our revenues or maintain or increase our profitability on an ongoing basis.
The COVID-19 epidemic may adversely affect our revenues, results of operations and financial condition and the market price of our common stock.
In retrospect, we believe our business and net revenues were adversely affected in 2020 and 2021 by lockdowns, travel-related restrictions and other governmental responses to the pandemic related to the COVID 19 pandemic which inhibited the ability of our sales force to visit doctors’ offices and clinics and may have adversely affected the willingness of SCD patients to seek the care of a physician or to comply with physician-prescribed care. Ongoing COVID-19 infections or
23
future official responses could cause a temporary or prolonged decline in our revenues and have a material adverse effect on our results of operations and financial condition. COVID-19 or governmental responses also may adversely affect the timing and conduct of clinical studies or the ability of regulatory bodies to consider or grant approvals with respect to Endari® or our prescription grade L-glutamine, or PGLG, drug candidates or oversee the development of our drug candidates, may further divert the attention and efforts of the medical community to coping with COVID-19 and variants and disrupt the marketplace in which we operate. For example, we experienced a temporary disruption in 2020 in patient enrollment in our Pilot/Phase I study of PGLG oral powder in diverticulosis. Any outbreak of COVID-19 among our executives or key employees or their families and loved ones could disrupt our management and operations and adversely affect the effectiveness of our management, Endari® sales, and results of operations and financial condition. The foregoing factors could also have an adverse effect on economic and business conditions and the broad stock market, in general, or the market price of our common stock in particular.
We may expend our limited resources to pursue a product candidate or indication and fail to capitalize on product candidates or indications for which there is a greater likelihood of commercial success.
Because we have limited financial and management resources, we are able to focus only upon a limited number of research programs and product candidates. As a result, we may forego or delay pursuit of opportunities with other product candidates or for other indications that later prove to have greater commercial potential. Our resource allocation decisions may cause us to fail to capitalize on viable product candidates or profitable market opportunities. Our spending on current and future research and development programs and product candidates for the specific indications we selected may not yield any commercially viable products. If we do not accurately evaluate the commercial potential or target market for a particular product candidate, we may relinquish valuable rights to that product candidate through collaboration, licensing or other arrangements in cases in which it would have been more advantageous for us to retain sole development and commercialization rights.
We face intense competition from companies with greater resources than us, and if our competitors are successful in marketing or develop alternative treatments, our commercial opportunities may be reduced or eliminated.
The pharmaceutical industry is characterized by rapidly advancing technologies, intense competition and a strong emphasis on developing proprietary therapeutics. We face competition from a number of sources, some of which may target the same indication as Endari®, such as pharmaceutical companies, including generic drug companies, biotechnology companies, drug delivery companies and academic and research institutions, many of which have greater financial resources, marketing capabilities, including well-established sales forces, manufacturing capabilities, research and development capabilities, experience in obtaining regulatory approvals for product candidates than do we. For example, in late 2019 the FDA approved a new drug application, or NDA, submitted by Novartis, permitting the marketing of ADAKVEO® (crizanlizumab-tmca) to reduce the frequency of vaso-occlusive crises in adults and pediatric patients aged 16 years and older with SCD. ADAKVEO®, which is administered by intravenous infusion every four weeks, is a selectin blocker humanized IgG2 kappa monoclonal antibody that binds to P-selectin. Also, in late 2019, Global Blood Therapeutics, Inc. which later acquired by Pfizer Inc., (“Pfizer”) announced that the FDA approved its NDA for Oxbryta™ (voxelotor) tablets for the treatment of SCD in adults and children 12 years of age and older. Oxbryta™ is an oral, once-a-day therapy intended to treat SCD by targeting hemoglobin polymerization. Both Novartis and Pfizer have far greater financial, sales and marketing resources than our company and there is no assurance that we will be able to compete effectively with ADAKVEO® or Oxbryta™ as a stand-alone therapy or that Endari® will gain widespread use as an adjunct to the use of ADAKVEO® or Oxbryta™. If we are unable to compete effectively or successfully position Endari® as a complementary therapy, our Endari® sales and results of operation may suffer, which could have a material, adverse effect on our financial condition. We also face competition from hydroxyurea and non-prescription grade L-glutamine supplements. Non-prescription grade L-glutamine is manufactured in large quantities, primarily by a few large chemical companies, and processed and sold as a nutritional supplement. The sale of non-prescription grade L-glutamine nutritional supplements, or generic prescription-grade or non-prescription grade L-glutamine products, at prices lower than the prices that we charge for Endari® could have a material adverse effect on our sales of Endari®, especially in the MENA region or other markets where we have no market exclusivity, and our results of operations and financial condition.
If we are unable to achieve and maintain adequate levels of coverage and reimbursement for Endari®, on reasonable pricing terms, its commercial success may be severely hindered.
Successful sales of Endari® depend on the availability of adequate coverage and reimbursement from third-party payors and governmental healthcare programs, such as Medicare and Medicaid. Patients who are prescribed medicine for the treatment of their conditions generally rely on third-party payors to reimburse all or a significant portion of the costs associated with their prescription drugs. Coverage determination depends on financial, clinical and economic outcomes that
24
often disfavors new drug products when more established or lower cost therapeutic alternatives are already available or subsequently become available. Although Endari® is reimbursable by the Centers for Medicare and Medicaid Services, and every state provides coverage for Endari® for outpatient prescriptions to all eligible Medicaid enrollees within their state Medicaid programs, the reimbursement amounts are subject to change and may not be adequate and may require higher co-payments that patients find unacceptable. Patients are unlikely to use Endari® unless reimbursement is adequate to cover a significant portion of the cost of Endari®. Future coverage and reimbursement will likely be subject to increased pressure in the U.S. Third-party coverage and reimbursement for Endari® may cease to be available or adequate in the U.S., which could have a material adverse effect on our business, results of operations, financial condition and prospects.
In addition, the market for Endari® will depend significantly on access to third-party payors’ drug formularies, which are lists of medications for which third-party payors provide coverage and reimbursement. The competition in the industry to be included in such formularies may lead to downward pricing pressures on us. Also, third-party payors may refuse to include Endari® in their formularies or otherwise restrict patient access to Endari® if a less costly generic equivalent or other alternative treatment is available.
The majority of Endari® sales are to a few customers and loss of a customer could adversely affect our results of operations.
We sell Endari® to specialty distributors and specialty pharmacies who, in turn, resell Endari® to pharmacies, hospitals and other customers. Four of our distributors account for approximately 79% of Endari sales in the year ended December 31, 2022, and the loss of any of these distributors or a material reduction in their Endari® purchases could have a material adverse effect on our business, results of operations, financial condition and prospects.
In addition, the distribution network for pharmaceutical products in the U.S. has undergone, and may continue to undergo, significant consolidation marked by mergers and acquisitions. As a result, a smaller number of large distributors control a significant share of the market, which has increased, and may continue to increase, competitive and pricing pressures on pharmaceutical products. There is no assurance that we can manage these pricing pressures or that specialty distributor and specialty pharmacy purchases will not fluctuate unexpectedly from period to period.
The market exclusivity for Endari® for SCD in the U.S. is limited and Endari® will have no market exclusivity in the Kuwait, Qatar or the United Arab Emirates, where Endari® is approved for marketing, the Kingdom of Saudi Arabia or other countries in the MENA region where applications for marketing approval are pending, which lack of exclusivity could adversely affect the commercial success of Endari® even if approved for marketing.
The exclusivity protections that protect Endari® for use for SCD are limited in ways that may affect our ability to effectively exclude third parties from competing against us. In particular:
These limitations and any reductions in our expected protection, including other products that could be approved by FDA under the Orphan Drug Act, may subject Endari® to greater competition than we expect and could adversely affect our ability to generate revenue from Endari®, perhaps materially. These circumstances may also impair our ability to obtain license partners or other international commercialization opportunities on terms acceptable to us, if at all.
Many of our potential customers are in markets with underdeveloped health care systems.
Our only approved product, Endari®, is a prescription-grade L-glutamine, or PGLG, oral powder treatment for sickle cell anemia and sickle ß0-thalassemia, two of the most common forms of SCD. SCD is a genetic blood disorder that affects 20 million to 25 million people worldwide and occurs primarily among those whose ancestors are from regions
25
including sub-Saharan Africa, South America, the Caribbean, Central America, the Middle East, India and Mediterranean regions such as Turkey, Greece and Italy. Thus, while SCD affects people throughout the world, the prevalence of SCD is higher in certain geographies, such as central and sub-Saharan Africa and the Caribbean, that currently have underdeveloped health care systems or significantly lower rates of health insurance coverage and incidence of these conditions in the United States is relatively low. Furthermore, many potential patients in many of these geographies are low-income and may be unable to afford Endari®. These factors may ultimately limit our addressable market. Our ability to achieve and sustain profitability may be adversely impacted if we are unable to access markets with greater prevalence of SCD or reach enough SCD patients in geographies with more well-developed health care systems.
A variety of risks associated with marketing Endari® internationally could hurt our business.
We recently received marketing authorization for Endari in Kuwait, Qatar and the United Arab Emirates and are seeking regulatory approval for Endari® for SCD in other countries in the MENA region, but may not be successful. For example, in January 2018, the European Medicines Agency, or EMA, provided their agreement on the pediatric investigation plan, or PIP, for our prescription grade L-glutamine oral powder in SCD and we filed with the EMA an application for marketing authorization, or MAA, in the EU. In May 2019, we announced that the EMA’s Committee for Medicinal Products for Human Use, or CHMP, had adopted a negative opinion regarding our MAA based upon the CHMP’s position that our main clinical study did not conclusively support the efficacy of the treatment in SCD patients. In light of the CHMP’s opinion, we withdrew our MAA in September 2019 to consider pursuing alternative decentralized and centralized regulatory pathways for obtaining marketing authorization in the EU or one or more EU countries. There is no assurance that we will be successful in obtaining marketing authorization in the EU or other jurisdictions outside the U.S. If we obtain marketing authorization, we expect that we will be subject to additional risks related to operating in foreign countries including:
These and other risks associated with international operations may compromise our ability to achieve or maintain profitability.
We may not be able to anticipate the demand for and appropriate supply of Endari®.
We monitor our distributors’ inventories of Endari® using a combination of methods. However, our estimates of distributor inventories may differ significantly from actual inventory levels. Significant differences between actual and our estimated inventory levels may result in excessive production (requiring us to hold substantial quantities of unsold inventory
26
which may result in the establishment of inventory reserves or actual write offs of expired inventory), inadequate supplies of products in distribution channels, insufficient product available at the retail level, and unexpected increases or decreases in orders from our specialty distributors. For example, as of December 31, 2022, we established a $5.0 million reserve against possible future inventory write offs. These changes may cause our revenues to fluctuate significantly from quarter to quarter, and in some cases may cause our operating results for a quarter to be below our expectations or the expectations of securities analysts or investors. In addition, we sometimes offer price discounts to our customers in advance of Endari® price increases, including a price increase implemented as of March 1, 2021, or as an incentive for bulk or advance orders of Endari®. Such discounts may result in specialty distributor purchases exceeding current demand, resulting in reduced specialty distributor purchases in later periods and substantial fluctuations in our results of operations from period to period. Sales attributable to one-time discounts offered by us increased in 2021, which adversely affected sales in subsequent periods. If our financial results are below analysts’ or investors’ expectations or cannot be reliably estimated, the market price of our common stock may be adversely affected.
If the L-glutamine manufacturer upon which we rely fails to produce in the volumes and quality that we require on a timely basis or fails to comply with stringent regulations applicable to pharmaceutical manufacturers, we may face interruptions in the commercialization of, or be unable to meet demand for, our L- glutamine based products, and may lose any marketing exclusivity and potential revenues.
We do not currently have our own manufacturing capabilities and depend upon a single Japanese supplier, Ajinomoto Aminoscience, LLC, or Ajinomoto, for commercial supplies of Endari® and clinical supplies of PGLG used in our product candidates under development. We intend to continue to rely on Ajinomoto to produce our PGLG, but we have not entered into, and may not be able to establish, long-term supply agreements with this key supplier on acceptable terms. Furthermore, pursuant to a letter of intent with Ajinomoto, we have indicated our willingness to purchase from Ajinomoto substantially all the L-glutamine that we will need for our commercial products. If Ajinomoto were to experience any manufacturing or production difficulties producing PGLG, or we were unable to purchase sufficient quantities of PGLG on acceptable terms, it could interrupt sales of Endari® and have a material, adverse effect on our financial condition and results of operations.
In addition, all manufacturers, packers, distributors and suppliers of pharmaceutical products must comply with applicable cGMP regulations for the manufacture of pharmaceutical products, which are enforced by the FDA through its facilities inspection program. If our manufacturers and key suppliers are not in compliance with cGMP requirements, it may result in a delay of approval for products undergoing regulatory review or the inability to meet market demands for any approved products, particularly if these sites are supplying single source ingredients required for the manufacture of any potential product. Furthermore, each manufacturing facility used to manufacture drug or biological products is subject to FDA inspection and must meet cGMP requirements. As a result, if one of the manufacturers that we rely on shifts production from one facility to another, the new facility must undergo a preapproval inspection and, for biological products, must be licensed by regulatory authorities prior to being used for commercial supply. A failure to comply with any applicable manufacturing requirements, including cGMP requirements, could delay or prevent the promotion, marketing or sale of our products. If the FDA or any other applicable regulatory authorities do not approve the facilities for the manufacture of Endari® or if they withdraw any such approval in the future, we may need to find alternative manufacturing facilities, which would significantly impact our ability to commercially supply Endari®.
If the safety of any quantities supplied is compromised due to a third-party manufacturer’s failure to comply with or adhere to applicable laws or for other reasons, we may be liable for injuries suffered by patients who have taken such products and we may not be able to obtain regulatory approval for or successfully commercialize our products.
We expect to rely on third parties to conduct future clinical trials of our product candidates and those third parties may not perform satisfactorily, including failing to meet deadlines for the conduct of such trials.
We engaged a third-party contract research organization (“CRO”) to conduct our clinical trials for Endari® and expect to engage a CRO to conduct any further required clinical trials of Endari® and any clinical trials with respect to any of our product candidates that may progress to clinical development. We expect to continue to rely on third parties, such as CROs, clinical data management organizations, medical institutions and clinical investigators, to conduct those clinical trials. Agreements with such third parties might terminate for a variety of reasons, including a failure to perform by the third parties. If we need to enter into alternative arrangements, it could delay our product development activities.
Our reliance on these third parties for research and development activities reduces our control over these activities but does not relieve us of our responsibilities. For example, we will remain responsible for ensuring that each of our clinical trials is conducted in accordance with the general investigational plan and protocols for the trial. Moreover, the FDA requires
27
us to comply with standards, commonly referred to as GCPs for conducting, recording and reporting the results of clinical trials to ensure that data and reported results are credible and accurate and that the rights, integrity and confidentiality of trial participants are protected. We also are required to register ongoing clinical trials and post the results of completed clinical trials on a government-sponsored database, www.ClinicalTrials.gov, within specified timeframes. Failure to do so can result in the FDA refusing to accept a NDA for the product candidate under study, fines, adverse publicity and civil and criminal sanctions.
Furthermore, these third parties may also have relationships with other entities, some of which may be our competitors. If these third parties do not successfully carry out their contractual duties, meet expected deadlines or conduct our clinical trials in accordance with regulatory requirements and our stated protocols, we will not be able to obtain, or may be delayed in obtaining, marketing approvals for our product candidates and will not be able to, or may be delayed in our efforts to, successfully commercialize them as products. We also expect to rely on other third parties to store and distribute supplies of our product candidates for clinical trials of them. Any performance failure on the part of our distributors could delay clinical development or marketing approval of our product candidates or commercialization of them as products, producing additional losses and depriving us of potential revenue.
Delays in the commencement, enrollment and completion of clinical trials could result in increased costs to us and delay in our ability to develop and obtain regulatory approval for product candidates. The commencement, enrollment and completion of clinical trials can be delayed for a variety of reasons, including delays or difficulties in enrolling patients due to unforeseen natural disasters, public health crises, political crises and other catastrophic events or other events outside of our control, such as the emergence and spread of COVID-19 and its variants, which may cause participants to not want to participate in these trials or otherwise have any unnecessary contact with the medical community.
Endari® may cause undesirable side effects or have other unexpected properties that could result in post-approval regulatory action.
The most common side effects seen with Endari® included constipation, nausea, headache, pain in the stomach area, cough, pain in the hands or feet, back pain, and chest pain. If we or others identify previously unknown undesirable side effects, or other previously unknown problems, caused by Endari® or other products with the same or related active ingredients, a number of potentially significant negative consequences could result, including:
Any of the above events resulting from undesirable side effects or other previously unknown problems could prevent us from achieving or maintaining market acceptance of Endari® and could substantially increase the costs of commercializing Endari®.
We face potential product liability exposure relating to Endari® and, if successful claims are brought against us, we may incur substantial liability if our insurance coverage for those claims is inadequate.
The commercial use of Endari® will expose us to the risk of product liability claims despite the fact it is approved for commercial sale by the FDA and manufactured in facilities licensed and regulated by the FDA. Any side effects, manufacturing defects, misuse or abuse associated with Endari® could result in injury to a patient or even death and product liability claims against us. In addition, a liability claim may be brought against us even if Endari® merely appears to have caused an injury. Product liability claims may be brought against us by consumers, health care providers, pharmaceutical companies or others selling or otherwise coming into contact with Endari® and we could incur substantial liabilities.
In addition, regardless of merit or eventual outcome, product liability claims may result in:
28
We maintain product liability insurance coverage and carry commercial excess and umbrella coverage, but our insurance coverage may not be sufficient to cover product liability related expenses or losses or cover us for any consequential expenses or losses we may suffer. We may not be able to continue to maintain insurance coverage at a reasonable cost, in sufficient amounts or upon adequate terms to protect us against losses due to product liability. Large judgments have been awarded in class action or individual lawsuits based on drugs that had unanticipated side effects, including side effects that are less severe than those of Endari®. Successful product liability claims against us could cause the value of our common stock to decline and, if judgments exceed our insurance coverage, reduce our cash and have a material adverse effect on our business, results of operations, financial condition and prospects.
The use of any of our product candidates in clinical trials and in the market may expose us to liability claims.
We are exposed to potential liability risks inherent in the testing and manufacturing of our product candidates and marketing of any products. While in clinical stage testing, our product candidates could potentially harm people or allegedly harm people and we may be subject to costly and damaging product liability claims. Informed consent and contractual limitations on payments for subject injury or waivers we obtain may not be enforceable and may not protect us from liability or the costs of product liability litigation. Although we carry clinical product liability insurance, it may not be sufficient to cover future claims.
In addition, in some cases the contractors on which we rely for manufacturing our product candidates may indemnify us for third-party claims brought against us arising from matters for which these contractors are responsible. We could be materially and adversely affected if we were required to pay damages or incur defense costs in connection with a claim outside the scope of indemnity or insurance coverage, if the indemnity is not performed or enforced in accordance with its terms, or if our liability exceeds the amount of applicable insurance or indemnity. In addition, there can be no assurance that insurance will continue to be available in amounts and on terms acceptable to us, if at all, to cover any potential claims or liabilities.
We will need to increase the size and complexity of our organization in the future, and we may experience difficulties in managing our growth and executing our growth strategy.
We will need to expand our scientific, sales and marketing, managerial, operational, financial and other resources to support our planned commercialization activities. Continued operations and growth require that we manage our commercialization activities for Endari® and product development efforts successfully and in a cost-effective manner. We will also need to continue to improve our operational, financial, management and regulatory compliance controls and reporting systems and procedures.
We will need to attract and retain sufficient talented employees and scientific collaborators.
Historically we have utilized, and continue to utilize, part-time outside consultants to perform certain tasks, including tasks related to accounting and finance, compliance programs, clinical trial management, legal and regulatory affairs, formulation development and other drug development functions. Our growth strategy related to Endari® may entail expanding our use of consultants to implement these and other tasks going forward. There can be no assurance that we will be able to manage our existing consultants or engage other competent consultants, as needed, on economically reasonable terms.
29
We rely heavily on Yutaka Niihara, M.D., M.P.H., our Chairman and Chief Executive Officer, and the loss of his services would have a material adverse effect upon our business and prospects.
Our success depends to a significant extent upon the continued services of Yutaka Niihara, M.D., M.P.H., our founder and Chairman and Chief Executive Officer. The loss of Dr. Niihara’s services could materially and adversely affect our business and prospects. We do not maintain key man life insurance on Dr. Niihara or any of our other executive officers.
Our business and operations may be adversely affected by information technology (“IT”) system failures or cybersecurity or data breaches.
We rely on IT networks and systems, including those of third-party service providers, to collect, process, store and transmit confidential information including, but not limited to, personal information and intellectual property for a variety of functions including, but not limited to, conducting clinical trials, financial reporting, data and inventory management. We also outsource certain services, including recruiting services, call center services, contract sales organization services and other ancillary services relating to the commercial marketing and sale of Endari® in the U.S., as well as significant elements of our IT security systems, as a result, our service providers have access to our confidential information.
Despite the implementation of security measures and recovery plans, our network and information systems and those of third-party service providers may be vulnerable to damage from computer viruses, cyberattacks, physical or electronic break-ins, service disruptions, and security breaches from inadvertent or intentional actions by our employees or vendors, or from attacks by malicious third parties. While we have not experienced any such system failure or security breach to date, if such an event were to occur, our operations may be disrupted, and we may suffer from economic loss, reputational harm, regulatory actions or other legal proceedings. Further, such breaches and other inappropriate access can be difficult to detect, and any delay in identifying them may lead to increased risks of the actions described above. We expect that risks and exposures related to cybersecurity breaches will remain high for the foreseeable future due to the rapidly evolving nature and sophistication of these threats.
We have identified significant deficiencies in our internal controls over financial reporting.
We have experienced historical material weaknesses in our internal controls over financial reporting, and in connection with the preparation of this Annual Report, our management concluded that there continue to be significant deficiencies in our disclosure controls and procedures as described in more detail in Part II – Item 9A “Controls and Procedures” in this Annual Report. We cannot guarantee when our disclosure controls and procedures will be fully effective or that we will not identify other material weaknesses in the future. Any material weaknesses in our internal control over financial reporting could result in errors in our consolidated financial statements, which could erode market confidence in our company, adversely affect the market price of our common stock and, in egregious circumstances, result in possible securities law claims based upon such financial statements.
Our business may be adversely impacted by the consequences of Russia's invasion of Ukraine.
The United States, the U.K. and the EU governments, among others, have instituted various sanctions and export-control measures in response to Russia's invasion of Ukraine, including comprehensive financial sanctions, targeted at Russia or designated individuals and entities with direct or indirect business interests or government connections to Russia or those involved in Russian military activities. Governments have also enhanced export controls and trade sanctions targeting Russia’s imports of goods. The duration and intensity of this conflict, or its possible spread, and its potential impact on our business or operations is uncertain, but it is possible that our business and operations could be adversely affected.
Risks Related to Our Intellectual Property
We may not be able to obtain and enforce intellectual property rights that cover our commercial activities or are sufficient to prevent third parties from competing against us.
Our success with respect to Endari® will depend, in part, on our ability to preserve our trade secrets and to prevent third parties from infringing upon our proprietary rights because we do not have (and will do not expect to be able to obtain) composition of matter patents or methods of use patents that cover Endari®. In particular, the patent for the use of L-glutamine to treat SCD expired in May 2016 and our license to the patent terminated. This means that our competitors are free to utilize processes, technologies and methods that were previously protected by the SCD patent to potentially develop competing products. While we have an Orphan Drug designation for the use of L-glutamine for the treatment of SCD in the U.S., our Orphan Drug exclusivity will expire in July 2024 and may be lost sooner if another L-glutamine product for the
30
same indication demonstrates clinical superiority. If our competitors develop alternative L-glutamine products, it may have a material, adverse effect on our business and results of operations.
In addition to seeking patents for our intellectual property, we also rely on trade secrets, including unpatented know-how, technology and other proprietary information, in our business. We seek to protect our trade secrets, in part, by entering into non-disclosure and confidentiality agreements with parties who have access to them, such as our employees, corporate collaborators, outside scientific collaborators, contract manufacturers, consultants, advisors and other third parties. Despite these efforts, any of these parties may breach the agreements and disclose our proprietary information, including our trade secrets, and remedies thereunder may not be adequate. Enforcing a claim that a party illegally disclosed or misappropriated a trade secret is difficult, expensive and time consuming, and the outcome is unpredictable. Some courts inside and outside the U.S. are less willing or unwilling to protect trade secrets. In addition, if any of our trade secrets were to be lawfully obtained or independently developed by a competitor, we would have no right to prevent them, or those to whom they communicate it, from using that technology or information to compete with us.
Although we expect all our employees to assign their inventions to us, and all our employees, consultants, advisors and any third parties who have access to our proprietary know-how, information or technology to enter into confidential information and invention agreements, we cannot provide any assurances that all such agreements have been duly executed or will be enforceable.
We depend on licenses of certain patents for the development of some of our product candidates. If any of these licenses terminate, or if any of the licensed patents is successfully challenged, we may be unable to continue the development of the affected product candidates.
Our ability to develop certain product candidates depends on an exclusive license we have obtained to patents that claim the use of Kainos’s KM10544 IRAK4 inhibitor to treat cancers. The license could be terminated if we fail to satisfy our obligations under it. In the event any claims in the patents that we have been licensed are challenged, the court or patent authority could determine that such patent claims are invalid or unenforceable or not sufficiently broad in scope to protect our proprietary rights. As the licensee of such patents, our ability to participate in the defense or enforcement of such patents could be limited.
If we are unable to protect proprietary technology that we invent and develop, we may not be able to compete effectively, and our business and financial prospects may be harmed.
Where appropriate, we seek patent protection for inventions we conceive and reduce to practice, however, patent protection may be limited or not available for all these inventions. In addition, we may need to design around patents held by others. If we must spend significant time and money protecting our patents, designing around patents held by others or in-licensing patent or other proprietary rights held by others, potentially for large fees, our business and financial prospects may be harmed.
The patent prosecution process is expensive and time consuming, and we may not be able to file and prosecute all necessary or desirable patent applications at a reasonable cost or in a timely manner. It is also possible that we will fail to identify patentable aspects of our research and development output before it is too late to obtain patent protection. We also may have to relinquish to strategic partners or other third parties to whom we license our technology the right to control the preparation, filing and prosecution of patent applications claiming our inventions and to maintain any resulting patents. Therefore, patent applications and patents claiming our inventions may not be prosecuted and enforced in a manner consistent with the best interests of our business.
Our pending and future patent applications may not result in patents being issued that protect our product candidates, in whole or in part, or which effectively prevent others from commercializing competitive product candidates. Changes in either the patent laws or interpretation of the patent laws in the U.S. and other countries may diminish the value of our patents or narrow the scope of our patent protection.
Even if our patent applications issue as patents, they may not issue in a form that will prevent competitors from competing with us or otherwise provide us with any competitive advantage. Our competitors may be able to circumvent our patents by developing similar or alternative treatments in a non-infringing manner.
In addition, the issuance of a patent is not conclusive as to its inventorship, scope, validity or enforceability, and our patents may be challenged in the courts or patent offices in the U.S. and abroad. Such challenges may result in loss of exclusivity, freedom to operate and/or in patent claims being narrowed, invalidated or held unenforceable, in whole or in part, which could limit our ability to prevent others from commercializing products similar or identical to our product candidates
31
or products, or limit the duration of the patent protection of our product candidates or products. Given the amount of time required for the development, testing and regulatory review of new therapeutics, patents protecting our product candidates might expire before or shortly after such candidates are commercialized as products. For example, our patent protection for Endari® expired in May 2016. As a result, our patent portfolio may not provide us with sufficient rights to exclude others from commercializing products similar or identical to ours.
Risks Related to Regulatory Oversight of Our Business and Compliance with Law
Endari® is subject to ongoing and continued regulatory review, compliance with which may result in significant expense and limit our ability to commercialize Endari®.
We are subject to ongoing FDA obligations and continued regulatory review with respect to the manufacturing, processing, labeling, packaging, distribution, adverse event reporting, storage, advertising, promotion and recordkeeping for Endari®. These requirements include submission of safety and other post-marketing information and reports, as well as continued compliance with good clinical practices and good laboratory practices or cGMPs. In addition, our product advertising and promotion are subject to regulatory requirements and continuing regulatory review. The FDA strictly regulates the promotional claims that may be made about prescription drug products. In particular, a drug product may not be promoted for uses that are not approved by the FDA as reflected in the product’s approved labeling, although the FDA does not regulate the prescribing practices of physicians.
Manufacturers of drug products and their facilities are subject to continual review and periodic inspections by the FDA and other regulatory authorities for compliance with cGMP regulations. If we or a regulatory agency discovers previously unknown problems with a product, such as adverse events of unanticipated severity or frequency, or problems with the facility where, or processes by which, the product is manufactured, a regulatory agency may impose restrictions on that product, the manufacturer or us, including requiring product recall, notice to physicians, withdrawal of the product from the market or suspension of manufacturing.
The FDA’s regulations, policies or guidance may change, and new or additional statutes or government regulations may be enacted that could further restrict or regulate post-approval activities relating to our commercialization of Endari®. We cannot predict the likelihood, nature or extent of adverse government regulation that may arise from future legislation or administrative action. If we are not able to achieve and maintain regulatory compliance, we may not be permitted to market Endari®, which would adversely affect our ability to generate revenue and achieve or maintain profitability.
We may not be able to receive eventual regulatory approval of PGLG treatment for diverticulosis or other indications, which would adversely affect our future prospects.
All our product candidates are still in preclinical or early-stage clinical development. Regulatory approval is required to market our PGLG treatment for diverticulosis or other indications and for any other product candidates we may develop. Even if the FDA and other regulatory authorities eventually approve our PGLG treatment for diverticulosis or any of our other product candidates, the manufacture, packaging, labeling, distribution, marketing and sale of such products will be subject to strict and ongoing post-approval regulations. Compliance with such regulations will be expensive and consume substantial financial and management resources.
The FDA has the authority to regulate the claims we make in marketing our prescription products to ensure that such claims are true, not misleading, supported by scientific evidence, and consistent with the approved labeling of those products. Failure to comply with FDA requirements in this regard could result in, among other things, warning letters, withdrawal of approvals, seizures, recalls, injunctions prohibiting a product’s manufacture and distribution, restricting promotional activities, requiring corrective actions regarding sales and marketing activities, other operating restrictions, civil money penalties, disgorgement, and criminal prosecution. In addition, if we make any marketing claims that are related to a health care provider’s unlawful submission for reimbursement from government programs, we could be subject to potential liability for violations of the False Claims Act, which may lead to disqualification from government programs or criminal prosecution, or both. Any of these government enforcement actions, if taken against us, could negatively impact our product sales and profitability.
Additionally, regulatory approval of any of our prescription products may be conditioned on our agreement to conduct costly post-marketing follow-up studies to monitor the safety or effectiveness of such products or to implement specific risk mitigation strategies. In addition, as clinical experience with any of our products following such approval, if any, expands after approval because the product is used by a greater number and more diverse group of patients than during clinical trials, unknown side effects or other problems may be observed that were not observed or anticipated during pre-approval clinical trials. In any such case, one or more regulatory authorities could require additional risk information be
32
added to the labeling of the product, restrict the indications for which the product may be sold, restrict the distribution channels, or revoke the product’s regulatory approval, which could hinder our ability to generate revenues from that product. If we fail to develop and commercialize our product candidates as planned, our financial results and financial condition will be adversely affected, we will have to delay or terminate some or all of our research product development programs, and we may be forced to cease operations.
The development process to obtain FDA approvals for new drugs therapies is very costly and time consuming and if we cannot complete our clinical trials in a cost-effective manner, our operations may be adversely affected.
Before obtaining marketing approval from regulatory authorities for the sale of any product candidate, we or a collaborator must complete preclinical development and then complete one or more extensive clinical trials to demonstrate the safety and effectiveness of the product candidate in humans. Clinical testing is expensive, difficult to design and implement, can take many years to complete and is uncertain as to outcome. Costs of clinical trials may vary significantly over the life of a development project owing, but not limited to, the following:
If we are unable to control the timing and costs of our clinical trials and conduct our trials and apply for regulatory approvals in a timely and cost-effective manner, our operations may be adversely affected.
Our product development costs will also increase if any regulatory agencies impose a clinical hold on any of our clinical studies or we experience delays in obtaining marketing approvals, particularly if we are required to conduct additional clinical studies beyond those that we submit in any NDA. We do not know whether any of our preclinical studies or clinical trials will begin as planned, will need to be restructured or will be completed on schedule, or at all. Significant preclinical study or clinical trial delays also could shorten any periods during which we may have the exclusive right to commercialize our approved product candidates or allow our competitors to bring products to market before we do, and thereby impair our ability to successfully commercialize our product candidates.
We may not be able to complete clinical trial programs for any of our product candidates successfully within any specific period or at all, and if such clinical trials take longer to complete than we project, our ability to execute our current business strategy will be adversely affected.
Clinical testing is expensive, difficult to design and implement, can take many years to complete, and is uncertain as to outcome. A failure of one or more clinical trials can occur at any stage of development. The outcome of preclinical testing and early clinical trials may not be predictive of the success of later clinical trials, and interim results of a clinical trial do not necessarily predict final results. Moreover, clinical data are often susceptible to varying interpretations and analyses, and many companies that have believed their product candidates performed satisfactorily in preclinical studies and clinical trials have nonetheless failed to obtain marketing approval of them.
33
Generally speaking, whether we complete our clinical trials in a timely manner, or at all, for any product candidate is dependent in part upon: (i) the date the applicable investigational new drug, or IND, becomes effective enabling us to commence the applicable clinical studies (which, under U.S. law, occurs no more than 30 days after the FDA receives the IND, unless the FDA places the IND on clinical hold, in which case the FDA may request us to provide additional data from completed preclinical studies or undertake additional preclinical studies, the latter of which could materially delay the clinical and regulatory development of the applicable product candidate); (ii) the engagement of clinical trial sites and clinical investigators; (iii) reaching an agreement with clinical investigators on acceptable clinical trial agreement terms, clinical trial protocols or informed consent forms; (iv) obtaining approval from the institutional review boards used by the clinical trial sites we seek to engage; (v) the rate of patient enrollment and retention; and (vi) the rate to collect, clean, lock and analyze the clinical trial database.
Clinical trials required for demonstration of substantial evidence of effectiveness and safety often require the enrollment of large numbers of patients, and suitable patients may be difficult to identify and recruit. Our ability to enroll sufficient numbers of patients in our clinical trials, especially when the disease or condition being studied is rare, depends on many factors, including the size of the relevant patient population, the nature and design of the protocol, the proximity of patients to clinical sites, the eligibility and exclusion criteria applicable for the trial, existence of competing clinical trials and the availability of already approved therapeutics for the indications being studied (whether or not such therapeutics are less safe or less effective than our product candidate under trial). If we fail to enroll and maintain the number of patients for which the clinical trial was designed, the statistical significance and/or statistical power of that clinical trial may be reduced which would make it harder to demonstrate that the product candidate being tested in such clinical trial is safe and effective for its intended use.
We may be required to suspend, repeat or terminate our clinical trials if they do not meet regulatory requirements, the results are negative or inconclusive, human subject protections are inadequate, the trials are not well designed, or clinical investigators fail to comply with all requirements for the conduct of trials under the applicable IND, any of which may result in significant negative repercussions on our business and financial condition.
We cannot market a pharmaceutical product in any jurisdiction until we have completed rigorous preclinical testing and clinical trials for that product, demonstrated the product’s safety and substantial evidence of effectiveness for its intended use, obtained the approval of the applicable regulatory authority for our proposed labeling of the product, and met the other requirements of such jurisdiction’s extensive regulatory approval process. Preclinical testing and the conduct of clinical trials are long and expensive. Data obtained from preclinical and clinical tests can be interpreted in different ways and could ultimately be deemed by regulatory authorities to be insufficient with respect to providing substantial evidence of effectiveness and safety required for regulatory approval, which could delay, limit or prevent regulatory approval. It may take us many years to complete the required testing of our product candidates to support an application for marketing approval and failure can occur at any stage during this process.
We cannot provide assurance that our preclinical testing and clinical trials will be completed successfully within any time period specified by us, or without significant additional resources or expertise provided by third parties to conduct such testing. We cannot provide assurance that any such testing will demonstrate that our product candidates meet regulatory approval requirements for safety and effectiveness or that any such product will be approved for a specific indication. Results from early clinical trials may not be indicative of the results that will be obtained in later-stage clinical trials or in the population of patients for whom the applicable product is prescribed following any approval. In addition, negative or inconclusive results from the clinical trials we conduct, or adverse events experienced by the patients in such clinical trials, could cause us to have to suspend, repeat or terminate the clinical trials. Clinical trials are subject to continuing oversight by governmental regulatory authorities and institutional review boards and must meet the requirements of these authorities including but not limited to requirements for informed consent, human subject protection and good clinical practices; and we cannot guarantee that we will be able to comply, or that a regulatory authority will agree that we have complied, with such requirements.
We rely on third parties, such as CROs, contract laboratories, regulatory consultants and data management companies to assist us in overseeing and monitoring clinical trials as well as to process the clinical data and manage test requests, which may result in delays or failure to complete trials, if the third parties fail to perform or meet applicable regulatory requirements and standards. A failure by us or any such third parties to comply with the terms and conditions of the protocol for any clinical study or the regulatory requirements for a product candidate or to complete the clinical trials for a product candidate in the projected time frame could significantly delay or increase the cost of our studies and have a material adverse effect on our business and financial condition.
34
There are significant requirements imposed on us and on clinical investigators who conduct clinical trials under an IND. Although we are responsible for selecting qualified clinical investigators, providing them with the information they need to properly conduct an investigation, ensuring proper monitoring of the investigations and that the investigations are conducted in accordance with the general investigational plan and protocols contained in the IND, we cannot ensure the clinical investigators will maintain compliance with all regulatory requirements at all times. The pharmaceutical industry has experienced cases where clinical investigators have been found to incorrectly record data, omit data, or even falsify data. We cannot ensure that the clinical investigators in our trial will not make mistakes or otherwise compromise the integrity or validity of data, any of which would have a significant negative effect on our ability to obtain marketing approval.
Changes in regulatory requirements and guidance or unanticipated events during our clinical trials may occur, which may result in necessary changes to clinical trial protocols, informed consents and clinical trial budgets, any of which changes could result in increased costs to us, delay our development timeline or reduce the likelihood of successful completion of the clinical trial.
Changes in regulatory requirements or the FDA’s interpretation of those requirements, which may be provided through guidance documents, or the occurrence of unanticipated events during our clinical trials could require us to amend clinical trial protocols, informed consent forms and trial budgets. If we experience delays in initiation, conduct or completion of any of our clinical trials, or if we terminate any of our clinical trials due to changes in regulatory requirements or guidance documents, unexpected and serious adverse events, or other unanticipated events, we may incur additional costs and have difficulty enrolling subjects or achieving clinical investigator or institutional review board acceptance of the changes and successfully completing the trial. Any such additional costs and difficulties could potentially materially harm the commercial prospects for our product candidates and delay our ability to generate product revenue.
There are various uncertainties related to the research, development and commercialization of Kainos’s KM10544 IRAK4 inhibitor to treat cancers and the cell sheet engineering regenerative medicine products we are developing which could negatively affect our ability to commercialize such products.
We have historically focused on the research and development of our PGLG treatment for SCD and have little or no experience in the research, development or commercialization of potential cancer treatments such as Kainos’s KM10544 IRAK4 inhibitor or cell sheet regenerative medicine products or any other biological product. We are not aware of any clinical trials of cell sheet regenerative products in the U.S. or of any biological products based on cell sheet engineering that have been approved by regulatory authorities in any jurisdiction. Such products must be manufactured in conformance with current cGMP requirements as well as Good Tissue Practice (“GTP”) requirements and demonstrate that they are safe, pure and potent to be effective for their intended uses to obtain FDA approval. The GTP requirements, which are specifically applicable to all cellular-based products, are intended to prevent communicable disease transmission. It is uncertain what type and quantity of scientific data would be required to support initiation of clinical studies or to sufficiently demonstrate the safety, purity and potency of cell sheet regenerative medicine products for their intended uses. Such uncertainties could delay our ability to obtain FDA approval for and to commercialize such products. In addition, the research and commercialization of cell sheet regenerative medicine products could be hindered if third-party manufacturers of such products are not compliant with cGMP, GTP, and any other applicable regulations. Any delay in the development of, obtaining FDA approval for, or the occurrence of any problems with third-party manufacturers of cell sheet regenerative medicine products would negatively affect our ability to commercialize such products.
We are subject to numerous complex regulations and failure to comply with these regulations, or the cost of compliance with these regulations, may harm our business.
The research, testing, development, manufacturing, quality control, approval, labeling, packaging, storage, recordkeeping, promotion, advertising, marketing, distribution, possession and use of Endari® are subject to regulation by numerous governmental authorities in the U.S. The FDA regulates drugs under the Federal Food, Drug and Cosmetic Act and implementing regulations. Noncompliance with any applicable regulatory requirements can result in refusal to approve products for marketing, warning letters, product recalls or seizure of products, total or partial suspension of production, prohibitions or limitations on the commercial sale of products or refusal to allow the entering into of federal and state supply contracts, fines, civil penalties and/or criminal prosecution. Additionally, the FDA and comparable governmental authorities have the authority to withdraw product approvals that have been previously granted. Moreover, the regulatory requirements relating to Endari® may change from time to time, and it is impossible to predict what the impact of any such changes may be.
35
Health care reform measures and changes in policies, funding, staffing and leadership at the FDA and other agencies could hinder or prevent the commercial success of Endari®.
In the U.S., legislative and regulatory changes to the healthcare system could affect our future results of operations and the future results of operations of our potential customers. For example, the Medicare Prescription Drug, Improvement, and Modernization Act of 2003 established a Part D prescription drug benefit, under which Medicare beneficiaries can obtain prescription drug coverage from private sector plans that are permitted to limit the number of prescription drugs that are covered in each therapeutic category and class on their formularies. If Endari® is not widely included on the formularies of these plans, our ability to market Endari® may be adversely affected.
Furthermore, there have been and continue to be initiatives at the federal and state levels that seek to reduce healthcare costs. In March 2010, President Obama signed into law the Patient Protection and Affordable Health Care Act of 2010, as amended by the Health Care and Education Affordability Reconciliation Act of 2010 (jointly, the “PPACA”), which includes measures to significantly change the way health care is financed by both governmental and private insurers. Among the provisions of the PPACA of importance to the pharmaceutical industry are the following:
36
Additionally, individual states have become increasingly aggressive in passing legislation and implementing regulations designed to control pharmaceutical product pricing, including price or patient reimbursement constraints, discounts, restrictions on certain product access, and marketing cost disclosure and transparency measures, and encourage importation from other countries and bulk purchasing. Legally mandated price controls on payment amounts by third-party payors or other restrictions could harm out business, results of operations, financial condition and prospects.
In addition, regional healthcare authorities and individual hospitals are increasingly using bidding procedures to determine what pharmaceutical products and which suppliers will be included in their prescription drug and other healthcare programs. This may reduce demand for Endari® or put pressure on our product pricing, which could negatively affect our business, results of operations, financial condition and prospects.
The commercial success of Endari® will depend, in part, upon the availability of coverage and reimbursement from third-party payors at the federal, state and private levels. Third-party payors include governmental programs such as Medicare or Medicaid, private insurance plans and managed care plans. These third-party payors may deny coverage or reimbursement for a product or therapy in whole or in part if they determine that the product or therapy was not medically appropriate or necessary. Also, third-party payors have attempted to control costs by limiting coverage through the use of formularies and other cost-containment mechanisms and the amount of reimbursement for particular procedures or drug treatments.
Additionally, given recent federal and state government initiatives directed at lowering the total cost of healthcare, Congress and state legislatures will likely continue to focus on healthcare reform, the cost of prescription drugs and the reform of the Medicare and Medicaid programs. While we cannot predict the full outcome of any such legislation, it may result in decreased reimbursement for prescription drugs, which may further exacerbate industry-wide pressure to reduce prescription drug prices. This could harm our ability to market Endari® and generate revenues. In addition, legislation has been introduced in Congress (the Affordable and Safe Prescription Drug Importation Act) that, if enacted, would permit more widespread importation or re-importation of pharmaceutical products from foreign countries into the U.S., including from countries where the products are sold at lower prices than in the U.S. Such legislation, or similar regulatory changes, could lead to a decision to decrease our prices to better compete, which, in turn, could adversely affect our business, results of operations, financial condition and prospects. It is also possible that other legislative proposals having similar effects will be adopted.
Furthermore, regulatory authorities’ assessment of the data and results required to demonstrate safety and efficacy can change over time and can be affected by many factors, such as the emergence of new information, including on other products, changing policies and agency funding, staffing and leadership. We cannot be sure whether future changes to the regulatory environment will be unfavorable to our business prospects.
If we fail to comply with federal and state healthcare laws, including fraud and abuse and health information privacy and security laws, we could face substantial penalties and our business, results of operations, financial condition and prospects could be adversely affected.
As a pharmaceutical company, even though we do not and will not control referrals of healthcare services or bill directly to Medicare, Medicaid or other third-party payors, certain federal and state healthcare laws and regulations pertaining to fraud and abuse and patients’ rights are and will be applicable to our business. We could be subject to healthcare fraud and abuse and patient privacy regulation by both the federal government and the states in which we conduct our business. The laws that may affect our ability to operate include:
37
Because of the breadth of these laws and the narrowness of the statutory exceptions and safe harbors available under the U.S. federal Anti-Kickback Statute, it is possible that some of our business activities could be subject to challenge under one or more of such laws. If we or our operations are found to be in violation of any of the laws described above or any other governmental regulations that apply to us, we may be subject to penalties, including civil and criminal penalties, damages, fines, exclusion from participation in U.S. federal or state health care programs, and the curtailment or restructuring of our operations. Any penalties, damages, fines, curtailment or restructuring of our operations could materially adversely affect our ability to operate our business and our financial results.
The FDA provides guidelines with respect to appropriate promotion and continuing medical and health education activities. Although we endeavor to follow these guidelines, the FDA or the Office of the Inspector General: U.S. Department of Health and Human Services may disagree, and we may be subject to significant liability, including civil and administrative remedies as well as criminal sanctions. In addition, management’s attention could be diverted, and our reputation could be damaged.
Although compliance programs can mitigate the risk of investigation and prosecution for violations of these laws, the risks cannot be eliminated entirely. Any action against us for violation of these laws, even if we successfully defend against it, could cause us to incur significant legal expenses and divert our management’s attention from the operation of our business. Moreover, achieving and sustaining compliance with applicable federal and state privacy, security and fraud laws may prove costly.
Even though we obtained Orphan Drug designation for Endari®, we may not be able to maintain Orphan Drug marketing exclusivity for Endari® or any of our other product candidates.
Regulatory authorities in some jurisdictions, including the U.S. and the EU, may designate therapeutic products under development for relatively small patient populations as “orphan drugs”. Under the Orphan Drug Act, the FDA may designate a therapeutic product as an Orphan Drug if it is intended to treat a rare disease or condition, which is generally defined as a patient population of fewer than 200,000 individuals in the U.S. We have obtained Orphan Drug designation from the FDA, which will expire July 7, 2024, and Orphan Medicinal designation from the EC for L-glutamine treatment for SCD, and we may seek Orphan Drug designation for our other product candidates. Generally, if a product candidate with an Orphan Drug designation subsequently receives the first marketing approval for the indication for which it has been granted such designation, the drug is entitled to a period of marketing exclusivity, which precludes the FDA or EC, as applicable, from approving another marketing application for the same product candidate prior to the expiration of that time period. The applicable period is seven years in the U.S. and ten years in the EU. The exclusivity period in the EU can be reduced to six years if the product no longer meets the criteria for Orphan Medicinal designation or if its commercialization is sufficiently profitable so that market exclusivity is no longer justified. Orphan Drug and Orphan Medicinal exclusivity may be lost if the FDA or EC determines that the request for designation was materially defective or if the manufacturer is unable to ensure enough of the product to meet the needs of patients with the rare disease or condition. In the U.S., Orphan Drug exclusivity may be lost if another L-glutamine product for the same indication demonstrates clinical superiority, such as a better safety or efficacy profile, in which case the FDA would be permitted to approve the third-party product. Orphan Drug exclusivity does not bar the FDA from approving another L-glutamine product for any other indication. Nor does Orphan Drug designation bar the FDA from granting Orphan Drug designation and approving another product such as Oxbryta, from Pfizer Inc. for treating SCD, for the same orphan disease or condition.
Any product candidate for which we obtain marketing approval would be subject to post-marketing regulatory requirements and limitations and could be subject to recall or withdrawal from the market, and we may be subject to penalties if we fail to comply with such regulatory requirements or if we experience unanticipated problems in commercializing any of our product candidates, when and if any of them are approved by regulators.
Any product candidate for which we obtain marketing approval, along with the collection and reporting of post-approval clinical data, manufacturing processes, labeling, advertising and promotional activities for the resulting product, will be subject to continual requirements of and review by the FDA and other regulatory authorities. These requirements include
38
submissions of safety and other post-marketing information and reports, establishment registration and product listing requirements, cGMP requirements relating to manufacturing, quality control, quality assurance and corresponding maintenance of records and documents, requirements regarding the distribution of samples to physicians and recordkeeping. Even if the FDA or other regulators outside the U.S. grant marketing approval to any of our product candidates, the approval may be subject to limitations on the indicated uses for which it may be marketed as a product or to the conditions of approval, including the requirement to implement a risk evaluation and mitigation strategy (“REMS”). If any of our product candidates receives marketing approval, the labeling (including the package insert) that must accompany its distribution as a product may limit its approved use, which could limit the total number of prescriptions written for such products.
In consultation with the FDA, Emmaus is designing clinical studies to generate data in stages to fulfill the post-marketing commitment for the current SCD indication of Endari®. These studies will require additional funding and are designed to include dosing and safety, particularly in those populations not yet given Endari®. On any future products, the FDA may also require additional costly post-marketing studies or clinical trials or surveillance to monitor the safety or effectiveness of any other approved product. The FDA closely regulates the post-approval marketing and promotion of therapeutic products to ensure they are marketed for the approved indications and in accordance with the provisions of the approved labeling, and that any marketing claims or communications by a person or company responsible for the manufacture and distribution of the product regarding off-label use are truthful and not misleading. If we market any of our products for indications that have not been approved in a manner that is considered misleading or not truthful, we may be subject to enforcement action for misbranding the product. Violations of the FDC&A relating to the promotion of prescription products may lead to investigations alleging violations of federal and state healthcare fraud and abuse laws, as well as state consumer protection laws. In recent years, several pharmaceutical companies have been or settled lawsuits for fined significant amounts for such violations.
In addition, later discovery of previously unknown adverse events or other problems with any of our product candidates that are approved for marketing as products, the contract manufacturers from which we obtain supplies of these products, the manufacturing processes they use to manufacture these products, or our or their failure to comply with regulatory requirements, may have negative consequences, including:
Noncompliance with applicable regulatory requirements regarding safety monitoring, also called pharmacovigilance, and with requirements related to the development of therapeutics for the pediatric population, can also result in significant financial penalties. Similarly, failure to comply with applicable regulatory requirements regarding the protection of personal information can also lead to significant penalties and sanctions.
39
Recently enacted and future legislation may increase the difficulty and cost for us to obtain marketing approval of our product candidates and then commercialize them as products and affect the prices we may obtain.
In the U.S. and some foreign jurisdictions, there have been a number of legislative and regulatory changes and proposed changes regarding the healthcare system that could prevent or delay marketing approval of our product candidates, restrict or regulate post-approval activities and affect our ability to profitably sell any product candidates for which we obtain marketing approval.
Among policy makers and payors in the U.S. and elsewhere, there is significant interest in promoting changes in healthcare systems with the stated goals of containing healthcare costs, improving quality and expanding access. In the U.S., the pharmaceutical industry has been a particular focus of these efforts and has been significantly affected by major legislative initiatives. In March 2010, President Obama signed into law the Patient Protection and Affordable Care Act (“PPACA”), which intended to broaden access to health insurance, reduce or constrain the growth of healthcare spending, enhance remedies against fraud and abuse, add new transparency requirements for the healthcare and health insurance industries, impose new taxes and fees on the health industry and impose additional health policy reforms.
Among the provisions of the PPACA of importance to us are:
In addition, other legislative changes have been proposed and adopted since the PPACA was enacted. These changes include aggregate reductions to Medicare payments to providers of up to 2% per fiscal year, starting in 2013. On March 1, 2013, the President signed an executive order implementing the 2% Medicare payment reductions, and on April 1, 2013, these reductions went into effect. In January 2013, President Obama signed into law the American Taxpayer Relief Act of 2012, which, among other things, reduced Medicare payments to several providers and increased the statute of limitations period for the government to recover overpayments to providers from three to five years. These new laws may result in additional reductions in Medicare and other healthcare funding, which could have a material adverse effect on customers for any of our products, and, accordingly, our financial operations. Further, there have been multiple attempts through legislative action and legal challenge to repeal or amend the PPACA, and we cannot predict the impact that such a repeal or amendment would have on our business and operations.
40
On November 20, 2020, the U.S. Department of Health and Human Services published a Final Rule entitled “Removal of Safe Harbor Protection for Rebates to Plans or PBMs Involving Prescription Pharmaceuticals and Creation of New Safe Harbor Protection,” referred to as the Rebate Rule, which amends the discount safe harbor by eliminating protection for price concessions, including rebates, that are offered by pharmaceutical manufacturers to plan sponsors, or pharmacy benefit managers under contract with them, under the Medicare Part D program and Medicare Advantage Plans, unless the price reduction is one required by law. Effective January 1, 2022, in advance of the calendar year 2022 Part D plan year, safe harbor protection will be eliminated for manufacturer rebates paid directly (or indirectly through a pharmacy benefit manager) to Part D prescription drug plans and Medicare Advantage prescription drug plans. Effective December 30, 2020, the Rebate Rule will establish two new safe harbors. The first new safe harbor will protect price reductions paid by manufacturers to prescription drug plans (including prescription drug plans offered by Medicare Advantage organizations) and Medicaid managed care organizations, which are fully reflected at the point-of-sale. The second new safe harbor will protect fair-market-value service fees paid to pharmacy benefit managers by manufacturers. This new rule could result in a change in incentives for health plans and PBMs in negotiating rebates and discounts with manufactures for preferred formulary placement. Because the rule is not yet in effect, at this time we cannot predict how these changes would impact our business and operations.
We expect that the PPACA, as well as other healthcare reform measures that may be adopted in the future, may result in more rigorous coverage criteria and in additional downward pressure on the price that we receive for any of our products. Any reduction in reimbursement from Medicare or other government-funded programs may result in a similar reduction in payments from private payors. The implementation of cost containment measures or other healthcare reforms may prevent us from being able to generate revenue, attain profitability or commercialize any of our products.
Legislative and regulatory proposals have been made to expand post-approval requirements and restrict sales and promotional activities for prescription medicines. We cannot be sure whether additional legislative changes will be enacted, or whether the FDA regulations, guidance or interpretations will be changed, or what the impact of such changes on the marketing approvals of our product candidates, if any, may be. In addition, increased scrutiny by the U.S. Congress of the FDA’s approval process may significantly delay or prevent marketing approval, as well as subject us to more stringent product labeling and post-marketing testing and other requirements.
Risks Related to Our Investment in EJ Holdings, Inc.
EJ Holdings has no revenues and is dependent on us to fund its business and operations, and there is no assurance that we can continue to provide needed funding or that EJ Holdings will be able to continue its activities.
EJ Holdings, Inc., or EJ Holdings, a Japanese corporation 40% owned by us, is engaged in seeking to refurbish and phase in its amino acid manufacturing plant in Ube, Japan with the objective of eventually obtaining regulatory clearances for the manufacture of PGLG in accordance with cGMP. EJ Holdings has had no revenues since its inception, has depended on loans from us to acquire the Ube plant and fund its operations and will continue to be dependent on loans from us or other financing unless and until its plant is activated and it can secure customers, including us, for its products. There is no assurance that we can continue to provide needed funding to EJ Holdings, or that needed funding will be available from other sources. EJ Holdings has no commitments or understandings regarding any additional funding. If EJ Holdings fails to obtain needed funding, it may need to suspend activities at the Ube plant. Under the asset purchase agreement by which EJ Holdings purchased the Ube plant, the seller has the right to repurchase the plant at the purchase price, plus certain taxes, paid by EJ Holdings if the plant does not become operational within a reasonable period of time (not to exceed five years). In that event, it is likely that we would lose some or all of our investment in EJ Holdings.
EJ Holdings may not be able to obtain needed financing or repay our loans, and our ownership interest in EJ Holdings may be diluted by additional financing.
As of December 31, 2022, we had loaned EJ Holdings a total of approximately $25.0 million, including approximately $5.3 million loaned in 2022, and EJ Holdings will continue to be reliant upon loans from us to fund its planned activities at the Ube plant unless and until it is able to secure additional debt or equity financing to fund such activities. EJ Holdings also will need to raise substantial debt or equity financing to fund the plant’s operations if the phase-in of the plant is completed, including, but not limited to, maintaining the physical plant and maintaining regulatory approvals for the manufacture of its products. To the extent EJ Holdings raises additional debt or equity financing from sources other than us, its ability to repay our loans may be adversely affected or our ownership interest may be diluted.
41
If EJ Holdings fails to reactivate its plant and obtain customers, it may not be able to sell its plant and property and we may lose our investment.
If EJ Holdings fails to reactivate the Ube plant or to secure customers for its products, it may need to sell its plant and property. There is no assurance that it will be able to do so at an attractive price or at all. Our loans to EJ Holdings are general unsecured obligations of EJ Holdings and we have no mortgage or other security interest in the plant or other property of EJ Holdings. Depending on the price at which the plant and property can be sold if it becomes necessary, EJ Holdings may be unable to repay our loans and its other secured or unsecured obligations, and we may lose some or all of our investment in EJ Holdings.
EJ Holdings is subject to risks inherent in a new business and may not be successful.
EJ Holdings was formed in February 2017 for the purpose of acquiring, owning and operating Kyowa’s phased-out amino acid manufacturing plant in Ube, Japan. EJ Holdings is engaged in seeking to refurbish and phase in the plant in order to eventually obtain clearances to reactivate the plant from regulatory authorities, including FDA and other regulatory approvals for the manufacture of PGLG in accordance with cGMP. Neither we nor EJ Holdings has experience operating a manufacturing plant or managing a manufacturing business, and there is no assurance that EJ Holdings will be successful in bringing the plant online on a timely basis, or at all, or if it does so that it will be able to secure customers for its products or successfully implement its business plan.
We do not control EJ Holdings, and EJ Holdings may engage in activities contrary to our best interests.
JIP owns 60% of EJ Holdings and is entitled to designate a majority of EJ Holdings’ board of directors, its Chief Executive Officer and outside auditors, and, as such, controls the management, business and operations of EJ Holdings. It is possible that EJ Holdings will engage in actions or business activities that we believe are inconsistent with the MOU and not in our best interests and that may have an adverse effect on the economic or strategic value of our ownership interest in EJ Holdings.
EJ Holdings retains discretion over its use of any funds that we provide to it.
We do not control EJ Holdings’ day-to-day operations. Accordingly, funds provided by us to EJ Holdings may be used by it in any manner its management deems appropriate, including making capital expenditures and paying of salaries and other compensation of its officers and other employees. There is no assurance that EJ Holdings will use our funds in a manner that will enhance the value of our ownership interest in EJ Holdings.
Risks Related to Our Securities
We have been delinquent in our past SEC reporting obligations and if we fail to timely file our future SEC reports, our security holders and prospective investors will not have current information regarding our financial statements and status of our business and operations and our common stock may no longer be eligible for quotation on the OTC Markets Group, Inc.
We were unable to timely file with the SEC our Annual Reports on Form 10-K for the years ended December 31, 2019 and December 31, 2020 and our Quarterly Reports on Form 10-Q for 2020 or our Quarterly Report for the quarter ended March 31, 2021. Our failure to timely file our periodic SEC reports adversely affects the ability of our security holders and prospective investors to have current information regarding our financial statements and status of our business and operations and is likely to have adversely affected the liquidity and trading prices of our common stock. Under applicable rules of the Financial Industry Regulatory Authority, or FINRA, our failure to timely our periodic reports with the SEC may result in the disqualification of our common stock for quotation on the OTC Markets Group, Inc. In such event, there may be no established trading market for our common stock unless and until we are in compliance with our SEC reporting obligations and our common stock once again becomes eligible for quotation on the OTC Markets Group, Inc. or is listed on a national securities exchange.
We have experienced, and may continue to experience, significant volatility in our stock price.
The trading price for our common stock has historically been volatile and traded at higher or lower prices that are seemingly uncorrelated with our results of operations, financial condition or prospects. Between January 1, 2022 and December 31, 2022, the closing sale price of our common stock as reported on the OTC Markets Group, Inc. ranged from a
42
low of $0.08 to a high of $1.56 and may continue to exhibit volatility. Factors such as the following may affect the volatility in our stock price:
Other factors which may affect our stock price include general economic conditions or changes in the economy, the financial markets or the pharmaceutical or biotechnology industries driven by extraordinary events such as the COVID-19 pandemic or the Russian invasion of Ukraine and the prosecution of the war in Ukraine. We may be particularly vulnerable to volatility caused by these conditions or events, as we have only a single approved product and have relatively thin trading volume in our common stock.
Trading on the OTC Markets is volatile and sporadic, which could depress the market price of our common stock and make it difficult for our investors and stockholders to resell their common stock.
Public quotations for our common stock are available on the OTCQX tier of the OTC Markets. Trading in securities quoted on the OTC Markets is often thin and characterized by wide fluctuations in trading prices due to many factors, some of which may have little to do with our operations or business prospects. This volatility could depress the market price of our common stock for reasons unrelated to our business or operating performance. Moreover, the OTC Markets is not a stock exchange, and trading of securities on the OTC Markets is often more sporadic than the trading of securities listed on a quotation system such as The Nasdaq Capital Market or a stock exchange like the NYSE American. These factors may result in investors having difficulty purchasing and reselling shares of our common stock.
Our outstanding warrants and convertible promissory notes may result in further dilution to our stockholders.
Certain of our outstanding warrants to purchase a total of up to approximately 4,038,200 shares of our common stock provide for a so-called full-ratchet anti-dilution adjustment in the event we sell or issue shares of common stock or common stock equivalents at an effective price less than the exercise price of such warrants, subject to certain exceptions. These anti-dilution adjustments resulted in a reduction in the exercise price of such warrants to $0.45 per share in February 2022 and to $0.37 a share in January, 2023 by reason of the conversion of an outstanding convertible promissory notes described below. As of December 31, 2022, we had outstanding approximately $14.1 million principal amount of convertible promissory notes which are convertible into shares of our common stock at a conversion price of $0.37 per share, subject to possible future reductions on a quarterly basis in the event the prevailing trading price of our common stock is less than the then-conversion price. The anti-dilution adjustments of our outstanding warrants would be triggered by future issuances by us of shares of our common stock upon conversion of the convertible promissory notes, or otherwise, at a price per share below the then-exercise price of such warrants, which adjustments would have a further dilutive effect on our stockholders.
Stockholders may experience future dilution from future equity offerings.
To raise additional capital in the future we may sell and issue additional shares of our common stock or securities convertible into or exchangeable for our common stock, which sales would have a dilutive effect on the percentage ownership of our existing stockholders.
A substantial number of shares of common stock may be sold in the market, which may depress the market price for our common stock.
Sales of a substantial number of shares of our common stock in the public market, or the possibility such sales upon the exercise or conversion of our outstanding warrants or convertible promissory notes, could cause the market price of our common stock to decline or serve to depress the market price of our common stock. A substantial majority of the outstanding shares of our common stock are, and the shares of common stock issuable upon the exercise of our outstanding warrants and other convertible securities or shares which may be sold in future offerings by us will be, freely tradable without restriction or further registration under the Securities Act.
43
Our common stock is not traded on a national securities exchange, which may adversely affect our ability to raise needed financing.
The OTC Markets is not a national securities exchange within the meaning of federal and state securities laws, so our common stock is not eligible for the exemption from state securities, or “blue sky,” laws for “covered securities” within the meaning of the National Securities Markets Improvement Act of 1996, which may adversely affect our ability to sell our securities to raise needed financing and increase transactions costs of such financing.
As long as our common stock is quoted on the OTC Markets, our stockholders may face significant restrictions on the resale of our common stock due to state “blue sky” laws.
Each state has its own securities laws, often called “blue sky” laws, which limit sales of securities to a state’s residents, unless the securities are registered in that state or qualify for an exemption from registration and govern the reporting requirements for broker-dealers doing business directly or indirectly in the state. Before a security is sold in a state, there must be a registration in place to cover the transaction, or the transaction must be exempt from registration. The applicable broker must also be registered in that state. As long as our common stock is quoted on the OTCQX, a determination regarding registration will be made by those broker-dealers, if any, who agree to serve as market-makers for our common stock. There may be significant state blue sky law restrictions on the ability of investors to sell, and on purchasers to buy, our common stock. You should therefore consider the resale market for our common stock warrants to be limited, as you may be unable to resell your common stock without the significant expense of state registration or qualification.
Our stockholders have authorized our board of directors to effect a reverse stock split of our common stock, but if the board does so it may not result in the intended benefits.
At the Annual Meeting of stockholders held on December 8, 2022, our stockholders approved an amendment to our restated certificate of incorporation to authorize our board of directors in its discretion to effect a reverse stock split of the outstanding shares of our common stock within one year following the Annual Meeting at a ratio of not less than 1-for-5 nor greater than 1-for-8. Our board of directors may choose to effect a reverse stock split for the purpose of facilitating the listing of our common stock to a national securities exchange such as the NYSE American or The Nasdaq Capital Market. Absent other factors, reducing the number of outstanding shares of our common stock through a reverse stock split would tend to increase the per share market price of our common stock. However, other factors, such as our financial results, market conditions and the market perception of our business may adversely affect the market price of our common stock and there can be no assurance that a reverse stock split, if completed, will result in the intended benefits, that the market price of our common stock will increase in proportion to the reduction in the number of shares of our common stock outstanding before the reverse stock split or that the market price of our common stock will not decrease in the future.
We may issue preferred stock in the future, and the terms of the preferred stock may reduce the value of our common stock.
We are authorized to issue up to 15,000,000 shares of preferred stock in one or more series. Our board of directors may determine the terms of future preferred stock offerings without further action by our stockholders. If we issue preferred stock, it could affect your rights or reduce the value of our outstanding common stock. Specific rights granted to future holders of preferred stock may include voting rights, preferences as to dividends and liquidation, conversion and redemption rights, sinking fund provisions, and restrictions on our ability to merge with or sell our assets to a third party.
ITEM 1B. UNRESOLVED STAFF COMMENTS
Not applicable.
ITEM 2. PROPERTIES
We lease office space under operating leases from unrelated entities. The rent expense for the years ended December 31, 2022 and 2021 was approximately $1,187,000 and $1,201,000, respectively.
We lease 21,293 square feet of office space for our headquarters in Torrance, California, at a base rental of $81,717 per month, which the lease will expire on September 30, 2026. We also lease 1,163 square feet of office space in Dubai, UAE, which leases will expire on June 19, 2023.
44
We believe our existing facilities are adequate for our current and planned future operations, and we expect to be able to renew the leases on commercially reasonable terms.
ITEM 3. LEGAL PROCEEDINGS
None.
ITEM 4. MINE SAFETY DISCLOSURES
Not applicable.
45
PART II
ITEM 5. MARKET FOR REGISTRANT’S COMMON STOCK, RELATED STOCKHOLDER MATTERS AND ISSUER PURCHASES OF EQUITY SECURITIES
Market Information
Public quotations for our common stock are available on the OTCQX tier of the OTC Markets. The ticker symbol for our common stock is “EMMA.” The information reported on the OTC Markets reflect inter-dealer prices, without retail mark-up, mark-down or commission and do not necessarily represent actual transactions.
Holders
As of March 15, 2023, we had approximately 389 stockholders of record.
Dividends
We have never paid cash dividends on our common stock and do not expect to do so in the foreseeable future. The decision whether to pay cash dividends on our common stock will be made by our board of directors in its discretion and will depend on our financial condition, operating results, capital requirements, the requirements for paying dividends under the Delaware General Corporation Law, and other factors that the board of directors considers relevant.
Securities Authorized for Issuance under Equity Compensation Plans
The following table provides information as of December 31, 2022, regarding compensation plans, including any individual compensation arrangements, under which our equity securities are authorized for issuance:
Plan Category |
|
Number of securities to be issued upon exercise of outstanding options, warrants and rights |
|
|
Weighted average exercise price of outstanding options, warrants and rights |
|
|
Number of securities remaining available for future issuance under equity compensation plans |
|
|||
Equity compensation plans approved by security holders |
|
|
4,000,000 |
|
|
$ |
— |
|
|
|
4,000,000 |
|
Equity compensation plans not approved by security holders |
|
|
1,365,189 |
|
|
$ |
4.76 |
|
|
|
— |
|
Recent Sales of Unregistered Securities
On December 8, 2022, the Company issued 25,000 shares of its common stock to an individual in exchange for consulting services rendered or to be rendered to the Company. The shares were issued without registration under the federal securities laws in reliance upon the exemption from registration under Section 4(2) of the Securities Act of 1933, as amended, for transactions not involving a public offering. The shares were issued to a single individual in a privately negotiated transaction not involving a general solicitation or advertising.
Additional Information
Copies of our annual reports, quarterly reports, current reports, and any amendments to those reports are available free of charge on the Internet at www.sec.gov and on our website at www.emmausmedical.com. Such reports are not part of this Annual Report or incorporated by reference herein. All statements made in any of our reports, including all forward‑looking statements, are made as of the date of such reports and we do not assume or undertake any obligation to update any of those statements or documents, except as required by law.
ITEM 6. [RESERVED]
Not required for a smaller reporting company.
46
ITEM 7. MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS
Forward‑Looking Statements
The following discussion of our financial condition and results of operations should be read in conjunction with our financial statements and the related notes, and the other financial information included in this Annual Report. This discussion contains forward‑looking statements based upon current expectations that involve risks and uncertainties. Our actual results may differ materially from those anticipated in these forward‑looking statements because of various factors, including those set forth under “Risk Factors” or in other parts of this Annual Report.
Company Overview
We are a commercial-stage biopharmaceutical company engaged in the discovery, development, marketing and sale of innovative treatments and therapies, primarily for rare and orphan diseases. Our lead product, Endari® (prescription-grade L-glutamine oral powder) is approved by the U.S. Food and Drug Administration, or FDA, to reduce the acute complications of sickle cell disease (“SCD”), in adult and pediatric patients five years of age and older. In April 2022, Endari® was approved by the Ministry of Health and Prevention in the United Arab Emirates, or U.A.E, in adults and pediatric patients five years of age and older. The approval of Endari® in the U.A.E. was the first granted outside the U.S. In November and December of 2022, we received marketing authorizations for Endari® in Qatar and Kuwait, respectively. Applications for marketing authorization for other Gulf Cooperation Council, or GCC, countries are pending. While the applications are pending, the FDA approval of Endari® can be referenced to allow access to Endari® on a named-patient basis.
Endari® is marketed and sold in the U.S. by our internal commercial sales team. Endari® is reimbursable by the Centers for Medicare and Medicaid Services, and every state provides coverage for Endari® for outpatient prescriptions to all eligible Medicaid enrollees within their state Medicaid programs. Endari® is also reimbursable by many commercial payors. We have agreements in place with the nation’s leading distributors as well as physician group purchasing organizations and pharmacy benefits managers, making Endari® available at selected retail and specialty pharmacies nationwide. In April 2022 we launched a telehealth solution to afford SCD patients’ direct access to Endari® remotely through a web portal managed by our strategic partners, including Asembia LLC, US Bioservices Corporation and UpScript IP Holdings, LLC.
As of December 31, 2022, our accumulated deficit was $252.3 million, and we had cash and cash equivalents of $2.0 million. We expect net revenues to increase as we expand our commercialization of Endari® in the U.S. and realize revenues in Kuwait, Qatar, the U.A.E. and perhaps other GCC countries. Until we can generate sufficient net revenues from Endari® sales, our future cash requirements are expected to be financed through loans from related parties, third-party loans, public or private equity or debt financings or possible corporate collaboration and licensing arrangements. We are unable to predict if or when we will become profitable.
Critical Accounting Estimates
Management’s discussion and analysis of financial condition and results of operations is based on our financial statements, which have been prepared in accordance with accounting principles generally accepted in the United States (“GAAP”). The preparation of these financial statements requires us to make estimates and judgments that affect the reported amounts of certain assets, liabilities and expenses. On an ongoing basis, we evaluate these estimates and judgments, including those described below. We base our estimates on our historical experience and on various other assumptions that we believe to be reasonable under the present circumstances. These estimates and assumptions form the basis for making judgments about the carrying values of assets and liabilities that are not readily apparent from other sources. Actual results may differ materially from these estimates.
While our significant accounting policies are more fully described in Note 2 of the Notes to Financial Statements included in this Annual Report, we believe that the accounting policies discussed below under “Revenues, net” are the most critical to assist you in fully understanding and evaluating our reported financial results and affect the more significant judgments and estimates that we use in the preparation of our financial statements.
Financial Overview
Revenues, net
We realize net revenues primarily from sales of Endari® to our distributors and specialty pharmacy providers. Distributors resell our products to other pharmacy and specialty pharmacy providers, health care providers, hospitals, and
47
clinics. In addition to agreements with these distributors, we have contractual arrangements with specialty pharmacy providers, in-office dispensing providers, physician group purchasing organizations, pharmacy benefits managers and government entities that provide for government-mandated or privately negotiated rebates, chargebacks and discounts with respect to the purchase of our products. These various discounts, rebates, and chargebacks are referred to as “variable consideration.” Revenue from product sales is recorded net of variable consideration.
Under the Accounting Standards Codification (“ASC”) 606, we recognize revenue when our customers obtain control of our product, which typically occurs on delivery. Revenue is recognized in an amount that reflects the consideration that we expect to receive in exchange for the product, or transaction price. To determine revenue recognition for contracts with customers within the scope of ASC 606, we perform the following: (i) identify the contract(s) with a customer; (ii) identify the performance obligations in the contract; (iii) determine the transaction price; (iv) allocate the transaction price to our performance obligations in the contract; and (v) recognize revenue when (or as) we satisfy the relevant performance obligations.
Management estimates variable consideration using the expected-value amount method, which is the sum of probability-weighted amounts in a range of possible transaction prices. Actual variable consideration may differ from our estimates. If actual results vary from the estimates, we adjust the variable consideration in the period such variances become known, which adjustments are reflected in net revenues in that period. The following are our significant categories of variable consideration:
Sales Discounts: We provide our customers prompt payment discounts and from time to time offer additional discounts to encourage bulk orders to generate needed working capital. Sales attributable to bulk discounts offered by us increased in 2021 and adversely affected sales in subsequent period.
Product Returns: We offer our distributors a right to return product principally based upon (i) overstocks, (ii) inactive product or non-moving product due to market conditions, and (iii) expired product. Product return allowances are estimated and recorded at the time of sale.
Government Rebates: We are subject to discount obligations under state Medicaid programs and the Medicare Part D prescription drug coverage gap program. We estimate Medicaid and Medicare Part D prescription drug coverage gap rebates based upon a range of possible outcomes that are probability-weighted for the estimated payor mix. These reserves are recorded in the same period the related revenues are recognized, resulting in a reduction of product revenues and the establishment of a current liability that is included as accounts payable and accrued expenses on our balance sheet. Our liability for these rebates consists primarily of estimates of claims expected to be received in future periods related to recognized revenues.
Chargebacks and Discounts: Chargebacks for fees and discounts represent the estimated obligations resulting from contractual commitments to sell products to certain specialty pharmacy providers, in-office dispensing providers, group purchasing organizations, and government entities at prices lower than the list prices charged to distributors. The distributors charge us for the difference between what they pay for the products and our contracted selling price to these specialty pharmacy providers, in-office dispensing providers, group purchasing organizations, and government entities. In addition, we have contractual agreements with pharmacy benefit managers who charge us for rebates and administrative fee in connection with the utilization of product. These reserves are established in the same period that the related revenues are recognized, resulting in a reduction of revenues. Chargeback amounts are generally determined at the time of resale of product by our distributors.
Cost of Goods Sold
Cost of goods sold consists primarily of expenses for raw materials, packaging, shipping and distribution of Endari®.
48
Research and Development Expenses
Research and development expenses consist of expenditures for new products and technologies consisting primarily of fees paid to contract research organizations (“CRO”) that conduct clinical trials of our product candidates, payroll-related expenses, study site payments, consultant fees and other related costs. The costs of later-stage clinical studies such as Phase 2 and 3 trials are generally higher than those of earlier studies. This is primarily due to the larger size, expanded scope, patient related healthcare and regulatory compliance costs, and generally longer duration of later-stage clinical studies.
Our contracts with CROs are generally based on time and materials expended, whereas study site agreements are generally based on costs per patient as well as other pass-through costs, including start-up costs and institutional review board fees. The financial terms of these agreements are subject to negotiation and vary from contract to contract and may result in uneven payment flows. Payments under some of these contracts depend on factors such as the successful enrollment of patients and the completion of clinical trial milestones.
Future research and development expenses will depend on any new product candidates or technologies that we may introduce into our research and development pipeline. In addition, we cannot predict which product candidates may be subject to future collaborations, when such arrangements will be secured, if at all, and to what degree, if any, such arrangements would affect our development plans and capital requirements.
Due to the inherently unpredictable nature of the drug approval process and the interpretation of the regulatory requirements, we are unable to estimate the amount of costs of obtaining regulatory approvals of Endari® outside of the U.S. or the development of our other preclinical and clinical programs. Clinical development timelines, the probability of success and development costs can differ materially from expectations and can vary widely. These and other risks and uncertainties relating to product development are described in this Annual Report under the headings “Risk Factors—Risks Related to Our Business” and “Risk Factors—Risks Related to Regulatory Oversight of our Business and Compliance with Law.”
General and Administrative Expense
General and administrative expense consists principally of salaries and related employee costs, including share‑based compensation for our directors, executive officers and employees. Other general and administrative expense includes facility costs, and professional fees and expenses for audit, legal, consulting, and tax services.
Selling Expenses
Selling expenses consist principally of salaries and related costs for personnel involved in the promotion, sales, and marketing of Endari®. Other selling cost include advertising, third party consulting costs, the cost of in-house sales personnel and travel-related costs. We expect selling expenses to increase as we acquire additional sales personnel to support the commercialization of Endari® in the U.S. and abroad.
COVID-19
In retrospect, we believe our business and net revenues were adversely affected in 2020 and 2021 by lockdowns, travel-related restrictions and other governmental responses to the pandemic related to the COVID 19 pandemic which inhibited the ability of our sales force to visit doctors’ offices and clinics and may have adversely affected the willingness of SCD patients to seek the care of a physician or to comply with physician-prescribed care. Ongoing COVID-19 infections or future official responses could cause a temporary or prolonged decline in our revenues and have a material adverse effect on our results of operations and financial condition. COVID-19 or governmental responses also may adversely affect the timing and conduct of clinical studies or the ability of regulatory bodies to consider or grant approvals with respect to Endari® or our prescription grade L-glutamine, or PGLG, drug candidates or oversee the development of our drug candidates, may further divert the attention and efforts of the medical community to coping with COVID-19 or variants and disrupt the marketplace in which we operate. For example, we experienced a temporary disruption in 2020 in patient enrollment in our Pilot/Phase I study of PGLG oral powder in diverticulosis. Any outbreak of COVID-19 among our executives or key employees or their families and loved ones could disrupt our management and operations and adversely affect the effectiveness of our management, Endari® sales, and results of operations and financial condition. The foregoing factors could also have an adverse effect on economic and business conditions and the broad stock market, in general, or the market price of our common stock, in particular. We intend to consider changes to our business to adapt to the new post-pandemic environment, including an increased focus on our telehealth solution.
49
Inflation
Inflation has not had a material impact on our expenses or results of operations over the past two years, but may result in increased manufacturing, research and development, general and administrative and selling expenses in the foreseeable future.
Environmental Expenses
The cost of compliance with environmental laws has not been material over the past two years and any such costs are included in general and administrative costs.
Inventories
Inventories consist of raw materials, finished goods and work-in-process and are valued on a first‑in, first‑out basis and at the lower of cost or net realizable value. Substantially all raw materials purchased during the years ended December 31, 2022 and 2021 were supplied by one supplier.
Notes Payable, Convertible Notes Payable and Warrants
From time to time, we obtain financing from the sale and issuance of promissory notes or other debt instruments with detachable stock purchase warrants, some of which notes or debt instruments are convertible into shares of our common stock and some of which are issued to related parties. We analyze all of the terms of our notes payable and promissory notes issued with warrants to determine the appropriate accounting treatment, including determining whether embedded derivatives (conversion features, detachable stock purchase warrants and right to purchase common stock) are required to be bifurcated and treated as discount, and the applicable classification of the notes payable and embedded derivative as debt, derivative liabilities, equity or temporary equity (i.e., mezzanine capital).
Direct and incremental costs associated with the issuance of note payables such as legal fees and broker fees, among others, paid to parties are recorded as a reduction of note payable on the consolidated balance sheets. Issuance costs and discounts are amortized over the term of the respective financing agreement using the effective interest methods. Amortization of these amounts is included as a components of interest expenses in the consolidated statements of operation.
Notes payable to related parties, interest expense and accrued interest to related parties are separately identified in our consolidated financial statements. We also disclose significant terms of all transactions with related parties in the notes to our consolidated financial statements.
Share‑based Compensation
We recognize compensation expense for share‑based compensation awards during the service term of the recipients of the awards. The fair value of share‑based awards is calculated using the Black‑Scholes‑Merton pricing model. The Black‑Scholes‑Merton model requires subjective assumptions regarding future stock price volatility and expected time to exercise, which greatly affect the calculated values. The expected term of awards granted is calculated using the simplified method allowed under the Securities and Exchange Commission (“SEC”) Staff Accounting Bulletin Nos. 107 and 110. The risk‑free rate used to value an award is based on the U.S. Treasury rate as of the date of the award that corresponds to the vesting period of the award.
Fair Value Measurements
We define fair value as the price that would be received to sell an asset or paid to transfer a liability in an orderly transaction between market participants at the measurement date in accordance with ASC 820. We measure fair value under a framework that provides a fair value hierarchy that prioritizes the inputs to valuation techniques used to measure fair value. The hierarchy gives the highest priority to unadjusted quoted prices in active markets for identical assets or liabilities (Level 1 measurements) and the lowest priority to unobservable inputs (Level 3 measurements). The three levels of the fair value hierarchy are described as follows:
Level 1: Inputs to the valuation methodology are unadjusted quoted prices for identical assets or liabilities in active markets.
Level 2: Inputs to the valuation methodology include:
50
If the asset or liability has a specified (contractual) term, the Level 2 input must be observable for substantially the full term of the asset or liability.
Level 3: Inputs to the valuation methodology that are unobservable and significant to the fair value measurement.
An asset’s or liability’s fair value measurement level within the fair value hierarchy is based on the lowest level of any input that is significant to the fair value measurement. Valuation techniques used need to maximize the use of observable inputs and minimize the use of unobservable inputs The fair value of our debt instruments is not materially different from their carrying values as presented. The fair value of our convertible debt instruments was determined based on Level 2 inputs. The carrying value of the debt was discounted based on allocating proceeds to other financial instruments within the arrangement as discussed in Note 7 to our consolidated financial statements.
Certain of our outstanding warrants contain price adjustment provisions and, consequently, are accounted for as liabilities that are remeasured at fair value on a recurring basis using Level 3 inputs. The Level 3 inputs in the valuation of warrants include expected term and expected volatility.
Related Party Transactions
For a discussion of related party transactions, refer to Note 12 of the Notes to Consolidated Financial Statement included elsewhere in this Annual Report, which information is incorporated herein by reference.
Equity method investment
The Company owns 40% of the capital shares of EJ Holdings, which is treated as a so-called variable interest entity, or "VIE," for financial accounting purposes. A VIE such as EJ Holdings is to be consolidated by the primary beneficiary of its business and operations if the beneficiary has both (1) the power to direct the activities of the VIE that most significantly impact the VIE’s economic performance and (2) the obligation to absorb losses of, or the right to receive benefits from, the VIE that could potentially be significant to the VIE. The Company does not meet the power criterion for consolidating EJ Holdings. Accordingly, the Company accounts for its variable interest in EJ Holdings under the equity method under which its interest in EJ Holdings’ net loss is recorded as net loss on equity method investment in our statements of operation.
EJ Holdings is engaged in seeking to refurbish and phase in its amino acid manufacturing plant in Ube, Japan with the objective of eventually obtaining regulatory clearances for the manufacture of PGLG in accordance with cGMP. As of December 31, 2022, we had loaned EJ Holdings a total of approximately $25.5 million, including approximately $5.3 million loaned in 2022. EJ Holdings has had no revenues since its inception, has depended on loans from us to acquire the Ube plant and fund its operations and will continue to be dependent on loans from us or other financing unless and until its plant is activated and it can secure customers, including us, for its products. There is no assurance that we can continue to provide needed funding to EJ Holdings, or that needed funding will be available from other sources. EJ Holdings has no commitments or understandings regarding any additional funding. If EJ Holdings fails to obtain needed funding, it may need to suspend activities at the Ube plant.
51
Financial Highlights
|
|
Years Ended December 31, |
|
|||||
|
|
2022 |
|
|
2021 |
|
||
CONSOLIDATED STATEMENTS OF OPERATIONS (in thousands) |
|
|||||||
REVENUES, NET |
|
$ |
18,390 |
|
|
$ |
20,610 |
|
COST OF GOODS SOLD |
|
|
2,588 |
|
|
|
3,312 |
|
GROSS PROFIT |
|
|
15,802 |
|
|
|
17,298 |
|
OPERATING EXPENSES |
|
|
|
|
|
|
||
Research and development |
|
|
1,725 |
|
|
|
4,110 |
|
Selling |
|
|
7,493 |
|
|
|
5,878 |
|
General and administrative |
|
|
13,170 |
|
|
|
13,438 |
|
Total operating expenses |
|
|
22,388 |
|
|
|
23,426 |
|
LOSS FROM OPERATIONS |
|
|
(6,586 |
) |
|
|
(6,128 |
) |
OTHER INCOME (EXPENSE) |
|
|
|
|
|
|
||
Loss on debt extinguishment |
|
|
(501 |
) |
|
|
(365 |
) |
Change in fair value of warrant derivative liabilities |
|
|
1,304 |
|
|
|
(432 |
) |
Change in fair value of conversion feature derivative, notes payable |
|
|
4,259 |
|
|
|
(1,906 |
) |
Loss on investment in convertible bond |
|
|
(133 |
) |
|
|
— |
|
Net loss on equity method investment |
|
|
(1,913 |
) |
|
|
(2,733 |
) |
Foreign exchange loss |
|
|
(2,662 |
) |
|
|
(2,017 |
) |
Interest and other income |
|
|
680 |
|
|
|
761 |
|
Interest expense |
|
|
(5,013 |
) |
|
|
(3,101 |
) |
Total other expense |
|
|
(3,979 |
) |
|
|
(9,793 |
) |
LOSS BEFORE INCOME TAXES |
|
|
(10,565 |
) |
|
|
(15,921 |
) |
Income tax provision |
|
|
60 |
|
|
|
25 |
|
NET LOSS |
|
$ |
(10,625.00 |
) |
|
$ |
(15,946.00 |
) |
NET LOSS PER COMMON SHARE - BASIC AND DILUTED |
|
$ |
(0.21 |
) |
|
$ |
(0.32 |
) |
WEIGHTED-AVERAGE COMMON SHARES OUTSTANDING |
|
|
49,439,867 |
|
|
|
49,253,156 |
|
Years ended December 31, 2022 and 2021
Net Income (Loss). Net loss decreased by $5.3 million, or 33%, to $10.6 million for the year ended December 31, 2022 compared to net loss of $15.9 million for the year ended December 31, 2021. The decrease was due primarily to a $5.8 million decrease in other expense as discussed below, and a $1.0 million decrease in operating expenses partially offset by a $2.2 million decrease in net revenues. As of December 31, 2022, we had an accumulated deficit of approximately $252.3 million. Our net loss for the year ended December 31, 2022 included approximately $1.9 million of net loss attributable to our equity method investment in EJ Holdings Inc., or EJ Holdings, a variable interest entity, or VIE. The loss attributable to our equity investment in EJ Holdings for the year ended December 31, 2021 was $2.7 million.
Revenues, Net. Net revenues decrease by $2.2 million, or 11%, to $18.4 million for the year ended December 31, 2022 compared to $20.6 million in 2021. Substantially all net revenues were attributable to Endari® sales. The decrease in net revenues was due to lower volume sales of Endari® in 2022 and a higher level of price discounts related to large volume orders in 2022 than in 2021. We expect net revenues to increase in the foreseeable future as we expand our distribution channels for Endari® in the U.S. and commercialization of Endari® in the MENA region.
Cost of Goods Sold. Cost of goods sold decreased by $0.7 million, or 22%, to $2.6 million for the year ended December 31, 2022 compared to $3.3 million in 2021 due primarily to a decrease of $0.6 million in establishment of inventory reserve relating to Endari® inventory with a shelf-life of less than two years.
Research and Development Expenses. Research and development expenses decreased by $2.4 million, or 58%, to $1.7 million for the year ended December 31, 2022 compared to $4.1 million in 2021. The decrease was primarily due to $0.5 million in cash and $0.5 million in shares of the common stock issued in 2021 under the agreement with Kainos Medicine, Inc. (“Kainos”) to lead the clinical development of Kainos’ patented IRAK4 inhibitor and a decrease of $0.5 million in expenses relating to a pharmacokinetic characteristic and safety study for Endari® in the U.S. and a clinical study in Europe. We expect our research and development expenses to increase if we undertake additional studies including post marketing commitment studies.
52
Selling Expenses. Selling expenses increased by $1.6 million, or 27%, to $7.5 million for the year ended December 31, 2022 compared to 5.9 million in 2021. The increase was due to increases of $0.9 million in consulting services, $0.3 million in promotional expenses, $0.2 million in travel related expenses and $0.2 million in sales team compensation. We expect that our selling expenses will continue to increase as we expand Endari® marketing and sales activities both in the U.S. and outside the U.S.
General and Administrative Expenses. General and administrative expense decreased by $0.3 million, or 2%, to $13.2 million for the year ended December 31, 2022 compared to $13.4 million in 2021. We expect general and administrative expenses to increase as we add additional sales and administrative personnel to support the commercialization of Endari outside of the U.S.
Other Income (Expense). Other expense decreased by $5.8 million, or 59%, to $4.0 million for the year ended December 31, 2022 compared to other expense of $9.8 million in 2021. The decrease was primarily due to a $6.2 million increase in income from change in fair value of conversion feature derivative and $1.7 million increase in income from change in fair value of warrant derivative liabilities partially offset by a $1.9 million increase in interest expense in 2022.
Income Tax (Expense). Income tax expenses remained consistent to $60,000 for the year ended December 31, 2022 compared to income tax expense of $25,000 in 2021. A valuation allowance for net deferred tax assets recorded when it is more likely than not that we will not realize these assets through future operations. The valuation allowance increased by approximately $2.7 million for the year ended December 31, 2022, while it increased by $4.0 million for the years ended December 31, 2021. As of December 31, 2022, and 2021, we had no unrecognized tax benefits or position which, in the opinion of management would be reversed if challenged by a tax authority.
Seasonality
There may be seasonal variations in our Endari® sales due to factors such as year-end holidays, severe winter weather conditions in certain regions of the U.S., seasonal conditions that may affect medical practices and provider activity, including influenza or the Covid-19 outbreaks that may inhibit patients from seeking treatment for their SCD or filling or refilling prescriptions for Endari® and possibly other factors relating to the timing of patient deductibles and co-insurance limits.
Liquidity and Capital Resources
Based on our losses to date, anticipated future net revenues and operating expenses, debt repayment obligations, funding commitment to EJ Holdings and cash and cash equivalents balance of $2.0 million as of December 31, 2022, we do not have sufficient operating capital for our business without raising additional capital. We realized a net loss of $10.6 million for the year ended December 31, 2022 and anticipate that we will continue to incur net losses for the foreseeable future and until we can generate increased net revenues from Endari® sales. While we anticipate increased net revenues as we continue to expand our commercialization of Endari® in the U.S. through telehealth and other initiatives, as well as in the MENA region, there is no assurance that we will be able to increase our Endari® sales or attain sustainable profitability or that we will have sufficient capital resources to fund our operations until we are able to generate sufficient cash flow from operations.
Our subsidiary, Emmaus Medical, Inc., or Emmaus Medical, is party a purchase and sale agreement with Prestige Capital Finance, LLC, or Prestige Capital, pursuant to which Emmaus Medical may offer and sell to Prestige Capital from time to time eligible accounts receivable in exchange for Prestige Capital’s down payment, or advance, to Emmaus Medical of 75% of the face amount of the accounts receivable, subject to a $7,500,000 cap on advances at any time. The balance of the face amount of the accounts receivable will be reserved by Prestige Capital and paid to Emmaus Medical, less discount fees of Prestige Capital ranging from 2.25% to 7.25% of the face amount, as and when Prestige Capital collects the entire face amount of the accounts receivable.
Liquidity represents our ability to pay our liabilities when they become due, fund our business operations, fund the operations and retrofitting of EJ Holdings’ amino acid production plant in Ube, Japan, and meet our contractual obligations, including our obligations to purchase API under our supply arrangements with Telcon, and execute our business plan. Our primary sources of liquidity are our cash balances at the beginning of each period, proceeds from our accounts receivable factoring arrangement with Prestige Capital and our similar sales of future receipts to other parties, proceeds from related-party loans and other financing activities. Our short-term and long-term cash requirements consist primarily of working capital requirements, general corporate needs, our contractual obligations to purchase API from Telcon, debt service under our convertible notes payable and notes payable and planned ongoing loan funding to sustain EJ Holdings’ operations. We
53
have no contractual commitment to provide funding to EJ Holdings, but plan to continue to do so in the foreseeable to the extent we have cash available for this purpose.
As of December 31, 2022, we had outstanding $17.3 million in principal amount of convertible promissory notes and $9.2 million in principal amount of other notes payable that are due within a year. Our minimum lease payment obligations were $4.0 million, of which $1.0 million was payable within 12 months.
Our API supply agreement with Telcon provides for an annual API purchase target of $5 million and a target “profit” (i.e., gross margin) to Telcon of $2.5 million. To the extent these targets are not met, Telcon may be entitled to payment of the shortfall or to offset the shortfall against the Telcon convertible bond and proceeds thereof that are pledged as collateral to secure our obligations. With our consent, in February 2022 Telcon retained cash collateral and made offsets against the outstanding balance of our Telcon convertible bond for shortfalls under the API supply agreement for 2020 and 2021.
Due to uncertainties regarding our ability to meet our current and future operating and capital expenses, there is substantial doubt about our ability to continue as a going concern for 12 months from the date of this filing, and the report of our independent public accounting firm on our financial statements as of and for the year ended December 31, 2022 included in Item 15 of this Annual Report contains a going concern explanatory paragraph.
Cash Flows
Net cash used in operating activities
Net cash used in operating activities increased by$ 3.8 million, or 305%, to $ 5.1million for the year ended December 31, 2022 from $1.3 million for the year ended December 31, 2021. The increase was primarily due to $2.9 million in repayments under our API supply agreement with Telcon.
Net cash used in investing activities
Net cash used in investing activities decreased by $4.0 million, or 63%, to $ 2.4 million for the year ended December 31, 2022 from $6.4 million for the year ended December 31, 2021. This decrease was primarily due to a $1.0 million decrease in loan payment to equity method investees and increase of $2.9 million proceeds from the deemed sale of a portion of the Telcon convertible bond resulting from the offset of target shortfalls discussed above.
Net cash from financing activities
Net cash from financing activities decreased by $0.2 million, or 2%, to $7.2 million for the year ended December 31, 2022 from net cash from financing activities of $7.4 million for the year ended December 31, 2021.
Off‑Balance‑Sheet Arrangements
We had no off-balance sheet arrangements in the periods presented.
54
ITEM 7A. QUANTITATIVE AND QUALITATIVE DISCLOSURES ABOUT MARKET RISK
Not required for a smaller reporting company.
ITEM 8. FINANCIAL STATEMENTS AND SUPPLEMENTARY DATA
The information required by this Item 8 is incorporated by reference to the information that begins on Page F‑1 of this Annual Report.
ITEM 9. CHANGES IN AND DISAGREEMENTS WITH ACCOUNTANTS ON ACCOUNTING AND FINANCIAL DISCLOSURE
None.
ITEM 9A. CONTROLS AND PROCEDURES
Evaluation of Disclosure Controls and Procedures
We are responsible for establishing and maintaining disclosure controls and procedures (“DCP”) designed to ensure that information required to be disclosed by us in the reports filed by us under the Securities Exchange Act of 1934, as amended, or the Exchange Act, is: (a) recorded, processed, summarized and reported within the time periods specified in the SEC’s rules and forms; and (b) accumulated and communicated to our management, including our principal executive and principal financial officers, to allow timely decisions regarding required disclosures. In designing and evaluating our DCP, we recognize that any controls and procedures, no matter how well designed and implemented, can provide only reasonable assurance of achieving the desired objectives.
We conducted an evaluation pursuant to Rule 13a‑15 of the Exchange Act of the effectiveness of the design and operation of our DCP as of December 31, 2022 under the supervision and with the participation of our management, including our Chief Executive Officer and Chief Financial Officer. Based on that evaluation, our Chief Executive Officer and Chief Financial Officer concluded that our DCP were not effective as of December 31, 2022.
Remediation of Previously Identified Material Weakness
As previously reported, in connection with the preparation of our consolidated financial statements as of December 31, 2021, our management identified ongoing material weaknesses (the “Material Weaknesses”) in our internal control over financial reporting. The Material Weaknesses related to inadequate financial closing process, segregation of duties, including access control over information technology, especially financial information, inadequate documentation of policies and procedures over risk assessments, internal control and significant account processes, and insufficient entity risk assessment processes.
Since identifying the Material Weaknesses, we took several steps to remediate the Material Weaknesses, including:
More recently, in 2022 we implemented an integrated cloud-based enterprise resource planning system to manage our financial information and replace our outdated financial accounting systems and software.
As a result of these actions, management has concluded that the Material Weaknesses identified in previous fiscal years have been remediated but that there continued to be significant deficiencies in our internal control over financial reporting as of December 31, 2022. In particular, our finance and financial accounting department is thinly staffed, and there are some areas
55
in which we lack formal policies and procedures. Management does not believe, however, that these significant deficiencies materially affect the accuracy of our financial statements.
Management’s Annual Report on Internal Control Over Financial Reporting
Our management is responsible for establishing and maintaining adequate internal control over financial reporting as defined in Rules 13a‑15(f) under the Exchange Act. Our internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with GAAP. Our internal control over financial reporting includes those policies and procedures that (i) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect our transactions and our dispositions of the assets, (ii) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that our receipts and expenditures are being made only in accordance with authorizations of our management and directors, and (iii) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of our assets that could have a material effect on the financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risks that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate. Under the supervision and with the participation of our management, including our Chief Executive Officer and Chief Financial Officer, we conducted an evaluation of the effectiveness of our internal control over financial reporting based on the criteria set forth in Internal Control—Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission. Based on this evaluation, our management concluded that our internal control over financial reporting was not effective as of December 31, 2022.
Attestation Report
This Annual Report does not include an attestation report of our independent registered public accounting firm regarding internal control over financial reporting. As a non-accelerated filer, we are not subject to the attestation requirement.
Changes in Internal Control Over Financial Reporting
Except as described above, based on the evaluation of our management as required by paragraph (d) of Rule 13a‑15 of the Exchange Act, we believe that there were no changes in our internal control over financial reporting that occurred during the quarter ended December 31, 2022 that have materially affected, or are reasonably likely to materially affect, our internal control over financial reporting.
ITEM 9B. OTHER INFORMATION
None.
ITEM 9C. DISCLOSURE REGARDING FOREIGN JURISDICTIONS THAT PREVENT INSPECTIONS
Not applicable.
56
PART III
ITEM 10. DIRECTORS, EXECUTIVE OFFICERS AND CORPORATE GOVERNANCE
Directors and Executive Officers
The following individuals constitute our board of directors and executive officers:
Name |
|
Age |
|
|
Position |
|
Yutaka Niihara, M.D., M.P.H. |
|
|
63 |
|
|
Chairman and Chief Executive Officer |
Willis C. Lee, M.S. |
|
|
62 |
|
|
Director, Chief Operating Officer |
Yasushi Nagasaki, C.P.A. |
|
|
55 |
|
|
Chief Financial Officer |
George Sekulich |
|
|
57 |
|
|
Senior Vice President of Global Commercialization and Chief Information Officer |
Charles Stark, Pharm.D. |
|
|
67 |
|
|
Senior Vice President of Medical Affairs, Clinical, Regulatory |
Wei Peu Zen |
|
|
70 |
|
|
Director |
Seah H. Lim, M.D., Ph.D. |
|
|
64 |
|
|
Director |
Ian Zwicker |
|
|
75 |
|
|
Director |
Background of Officers and Directors
The following is a summary of the background of each of our directors and executive officers. Except as noted in their respective biographies below, each of our directors and officers became a director or officer as of the completion of our merger transaction with EMI Holding, Inc., or EMI Holding, on July 17, 2019. All directors serve until the next annual meeting of stockholders at which their successor is elected or their earlier resignation or removal as a director. One or more of our directors or officers also serve as directors or officers of one or more of our wholly owned subsidiaries.
Yutaka Niihara, M.D., M.P.H. served as Chairman and Chief Executive Officer since January 2016, as Chief Scientific Officer from April 2015 until December 2015, as President and Chief Executive Officer from April 2011 to April 2015 and as a director since April 2011 of EMI Holding, and as a director of EMI Holding’s predecessor, Emmaus Medical, from 2003 to April 2011. Since May 2005, Dr. Niihara has also served as the President, Chief Executive Officer and Medical Director of Hope International Hospice, Inc., or Hope Hospice, a Medicare-certified hospice program. From June 1992 to October 2009, Dr. Niihara served as a physician specialist for Los Angeles County. Dr. Niihara is the principal inventor of the patented L-glutamine treatment for SCD. Dr. Niihara has been involved in patient care and research for sickle cell disease during most of his career and is a widely published author on sickle cell disease. Dr. Niihara is board-certified by the American Board of Internal Medicine/Medical Oncology and by the American Board of Internal Medicine/Hematology. He is licensed to practice medicine in both the United States and Japan. Dr. Niihara is a Professor of Medicine at the David Geffen School of Medicine at UCLA. Dr. Niihara a holds B.A. degree in Religion from Loma Linda University, a M.D. degree from the Loma Linda University School of Medicine and a M.P.H. degree from Harvard School of Public Health. We believe Dr. Niihara is qualified to serve as a director due to his critical involvement in the research and development of Endari® and extensive knowledge and experience in treating sickle cell disease in the primary care setting.
Willis C. Lee, M.S. served as Chief Operating Officer since May 2011, as a director since December 2015, as Vice-Chairman of the board of directors since January 2016 and as Chief Financial Officer from October 2016 to July 2018 of EMI Holding. Mr. Lee also previously served as a director of EMI Holding from May 2011 to May 2014 and again from to December 2015 to January 2016. Mr. Lee served as the Co-Chief Operating Officer and Chief Financial Officer and as a director of Emmaus Medical from March 2010 to May 2011. Prior to that time, he was the Controller at Emmaus Medical from February 2009 to February 2010. From 2004 to 2010, Mr. Lee led worldwide sales and business development of Yield Dynamics product group at MKS Instruments, Inc., a provider of instruments, subsystems, and process control solutions for the semiconductor, flat panel display, solar cell, data storage media, medical equipment, pharmaceutical manufacturing, and energy generation and environmental monitoring industries. Prior to that time, Mr. Lee held various managerial and senior positions at various public and private companies in the semiconductor and other industries. Mr. Lee received his B.S. degree and a M.S. degree in Physics from University of Hawaii and University of South Carolina, respectively. We believe Mr. Lee is qualified to serve as a director due to his extensive knowledge and experience, as well as his intimate knowledge of the company through his service as an executive officer of the company and Emmaus Medical.
Yasushi Nagasaki, C.P.A. has served as Chief Financial Officer since September 1, 2020 and served as our Senior Vice President Finance from July 2019 to August 2020. Mr. Nagasaki also served as Senior Vice President Finance from April 2012 to July 2019 and as Chief Financial Officer from May 2011 to April 2012 of EMI Holding, with which we merged in July 2019. From September 2005 until joining EMI Holding, Mr. Nagasaki was the Chief Financial Officer of
57
Hexadyne Corporation, an aerospace and defense supplier. Mr. Nagasaki also served on the board of directors at Hexadyne Corporation from September 2005 to April 2011. From May 2003 to August 2005, Mr. Nagasaki was the Controller at Upsilon Intertech Corporation, an international distributor of defense and aerospace parts and subsystems. Mr. Nagasaki is a Certified Public Accountant and received a B.A. in Commerce from Waseda University and a M.A. in International Policy Studies from the Monterey Institute of International Studies, a graduate school of Middlebury College.
George Sekulich served as Senior Vice President of Global Commercialization and Chief Information Officer of EMI Holding Since May 2019, responsible for overseeing the commercial launch of Endari® in the United States. More recently, he has been engaged in laying the groundwork for the launch of Endari® and Xyndari® in overseas markets, with a special emphasis on the MENA region. Prior to becoming Senior Vice President of Global Commercialization, Mr. Sekulich served since September, 2014 as Chief Information Officer of EMI Holdings. Mr. Sekulich has over 25 years of experience and training in computer information services and is active in the design and support of our computer information systems. Prior to joining EMI Holding, Mr. Sekulich was the owner and operator of Magellan Net, a software provider services company. Mr. Sekulich received a B.S. in Computer Information Systems Management from California State University Dominguez Hills.
Charles Stark, Pharm.D. was appointed as Senior Vice President of Medical Affairs, Clinical, Regulatory on November 23, 2021, and served as our Senior Vice President of Research and Development since July 19, 2019 and in the same capacity with EMI Holding since 2013. He has more than 30 years of experience in medical affairs, research and academia. Previously, Dr. Stark was Director of Clinical Development at Bavarian Nordic, an immunotherapeutic company, and prior to that Associate Director of Medical Affairs for the Dendreon Corporation, an immunotherapeutic company. He has served as, Director, Medical Science Liaisons (cardiovascular, metabolic and oncology) at Pfizer, Inc., a pharmaceutical company. Dr. Stark has served as the Director of Investigational Drug Services and Clinical Research at LA BioMed at Harbor UCLA and at the Health Research Association at USC Medical Center. He has also served as a faculty member at the University of Southern California School of Pharmacy. Dr. Stark received his Pharm.D. from the University of Southern California and completed his residency at the Veteran’s Affairs Medical Center in West Los Angeles.
Wei Peu Zen is the Vice Chairman and Chief Executive Officer of Wai Kee Holdings Limited, a Hong Kong-based construction and infrastructure company whose shares are listed on the Main Board of Hong Kong Stock Exchange. He is also the Chairman, Chief Executive Officer and Managing Director of Build King Holdings Limited, a subsidiary of Wai Kee Holdings Limited. In addition, he is the Chairman of Road King Infrastructure Limited, an associated corporation of Wai Kee Holdings Limited. The shares of both Build King Holdings Limited and Road King Infrastructure Limited are listed on the Main Board of Hong Kong Stock Exchange. Mr. Zen has over 45 years of experience in civil engineering and is responsible for the overall management of Wai Kee Group and oversees the operations of Wai Kee Group. Mr. Zen holds a B.Sc. degree in Engineering from The University of Hong Kong and a M.B.A. degree from The Chinese University of Hong Kong and is a member of both the Institution of Civil Engineers and the Hong Kong Institution of Engineers and a fellow member of the Institute of Quarrying, UK. He is a past Honorary Treasurer of Hong Kong Construction Association and a member of HKTDC Infrastructure Development Advisory Committee. He is also the President of Hong Kong Contract Bridge Association. We believe Mr. Zen is qualified to serve as a director due to his executive experience and business expertise. Mr. Zen also brings to the board of directors his diverse experience as a foreign national and board member and executive officer of Hong Kong-based publicly traded companies.
Seah H. Lim, M.D., Ph.D, was appointed as a director on October 4, 2022 and has more than 25 years of experience working in academia and with pharmaceutical companies in the clinical developments of products in hematology, oncology, and transplantation. He is board-certified in Internal Medicine, Hematology, and Medical Oncology and is an internationally recognized physician-investigator with extensive leadership experience and a track record of success in clinical and research and development. Most recently, since June 2021 he has served as Chief Executive Officer of Medicovestor Bio PLC, Kuala Lumpur, Malaysia, a privately held development-stage biotechnology company. From January 2017 to December 2021, he served as a consultant to Salix Pharmaceuticals/Bausch Healthcare where he was instrumental in obtaining FDA designation of rifaximin as an orphan drug for the treatment of sickle cell disease. He also has served as a consultant to numerous “big pharma” companies, including Genzyme, USA, Burroughs Wellcome, and Amgen Corporation. Since October 2021, he has served as Associate Director, Allogenic Stem Cell Transplant and Director of the Adult Sickle Cell Program at Upstate State University of New York Medical Center, Syracuse, New York. Dr. Lim has authored or co-authored numerous peer-reviewed publications and has served as Section Editor, Journal of Translational Medicine since 2016. He received his MB ChB and MD degrees from Aberdeen University School of Medicine, Aberdeen, Scotland, and Ph.D. from University of Wales College of Medicine, Cardiff, Wales. We believe Dr. Lim is well-qualified to serve as a director based on his expertise and experience in the treatment of sickle cell disease and extensive background as a researcher and executive officer and consultant in the pharmaceutical industry both in the U.S. and abroad.
58
Ian Zwicker was appointed as a director on October 4, 2022. He previously served as a director, Chair of the Compensation Committee and member of the Governance and Nominations Committee of our Board of Directors from the completion of our merger transaction with EMI Holding, Inc. on July 17, 2019, until his retirement as a director in conjunction with our Annual Meeting of Stockholders held on November 23, 2021. He had served as a director of EMI Holding, Inc. since December 7, 2015. Mr. Zwicker is the founder of Zwicker Advisory Group, an independent financial advisory consulting firm, and has been its Chief Executive Officer since 2014. From 1981 to 1990, Mr. Zwicker served as Managing Director and held a variety of management positions at the investment banking firms of SG Cowen and Hambrecht & Quist. From 1990 to 1999, Mr. Zwicker served as Managing Director and head of worldwide technology investment banking for Donaldson, Lufkin & Jenrette Securities Corporation, and from 2000 to 2001 as the President of WR Hambrecht + Co (WRH). He was a Director of Stirling Energy Systems, Inc. from 2006 to 2012. Mr. Zwicker was a Partner at WRH and was also Head of Capital Markets from 2013 to 2014. We believe Mr. Zwicker is qualified to serve as a director due to his prior service on the Board of Directors and standing Board committees and his extensive investment banking and financial expertise and experience.
Family and Other Relationships
There are no family relationships among any of our officers or directors.
Mr. Zen was originally appointed to the board of directors of EMI Holding on June 18, 2018 pursuant to the terms of outstanding convertible promissory notes dated November 6, 2017 and January 15, 2018 held by Mr. Zen and Wealth Threshold Limited, respectively, which entitled the note holders to designate one director if the aggregate investment in EMI Holding by the note holders and related note holders exceeded $20 million.
Board of Directors and Committees and Director Independence
Our board of directors currently consists of five members. Our board of directors has determined that each of Wei Peu Zen, Seah Lim and Ian Zwicker is an “independent” director as defined by The NASDAQ Marketplace Rules currently in effect and all applicable rules and regulations of the SEC. Mr. Zwicker, the sole member of the Audit Committee satisfies the “independence” standards of The NASDAQ Marketplace Rules applicable to members of such committee. The board of directors made this affirmative determination regarding these directors’ independence based on discussions with the directors and its review of the directors’ responses to a standard questionnaire regarding employment and compensation history, affiliations, family and other relationships and transactions between each director or any member of his or her immediate family and the Company or its subsidiaries or affiliates.
Audit Committee
Ian Zwicker is the sole Audit Committee member and an independent director as defined by The NASDAQ Marketplace Rules. Mr. Zwicker qualifies as an “audit committee financial expert” as defined under Item 407(d) of Regulation S‑K. The purpose of the Audit Committee is to represent and assist our board of directors in its general oversight of our accounting and financial reporting processes, audits of the financial statements and internal control and audit functions. The Audit Committee’s primary responsibilities and duties are to:
The board of directors has adopted a written charter for the Audit Committee. A copy of the Audit Committee Charter is available on our website at www.emmausmedical.com.
59
Governance and Nominations Committee and Compensation Committee
Our board of directors previously established both a Governance and Nominations Committee and a Compensation Committee, but the activities of the Committees have been suspending pending the possible eventual up listing of our common stock to a national securities exchange. In the meantime, our board of directors as a whole is responsible for the functions of the former Committees.
Section 16(a) Beneficial Ownership Reporting Compliance
Our common stock is currently registered under Section 12 of the Securities Exchange Act of 1934, as amended. As a result, and pursuant to Rule 16a‑2, our directors and executive officers and beneficial owners of 10% or more of our common stock are currently required to file statements of beneficial ownership with respect to their ownership of our equity securities under Sections 13 or 16 of the Exchange Act. Based on a review of written representations from our executive officers and directors and a review of Forms 3 and 4 and any Forms 5 furnished to us, we believe that during the fiscal year ended December 31, 2022 our directors and officers filed, on a timely basis, all reports required by Section 16(a) of the Exchange Act.
Code of Conduct and Ethics
Our board of directors has approved a Code of Conduct and Ethics, which we refer to as the Code of Ethics, which applies to our directors, officers and employees. The Code of Ethics addresses, among other things, honesty and ethical conduct, conflicts of interest, compliance with laws, regulations, and policies, including disclosure requirements under the federal securities laws, confidentiality, trading on inside information, and reporting of violations of the Code of Ethics. A copy of the Code of Ethics is available on our website at www.emmausmedical.com. Requests for copies of the Code of Ethics should be sent to Emmaus License Sciences, Inc., Attention: Secretary, 21250 Hawthorne Boulevard, Suite 800, Torrance, California 90503.
Insider Trading Policy
The Company has adopted insider trading policies and procedures governing the purchase, sale and other disposition of the Company’s securities, a copy of which is included as Exhibit 19 to this Annual Report.
ITEM 11. EXECUTIVE COMPENSATION
Summary Compensation Table
The following table sets forth information concerning the compensation earned by our Chief Executive Officer, and our two other most highly compensated executive officers, whom we refer to as our “named executive officers,” for the fiscal years ended December 31, 2022 and 2021:
Name and Position |
|
Year ended December 31 |
|
Salary |
|
|
Bonus |
|
|
Stock Awards |
|
|
Option |
|
|
|
All Other Compensation |
|
|
Total |
|
|||||||
Yutaka Niihara, M.D., MPH |
|
2022 |
|
$ |
385,000 |
|
|
$ |
— |
|
|
$ |
— |
|
|
$ |
— |
|
|
|
$ |
— |
|
|
$ |
385,000 |
|
|
Chairman and Chief Executive Officer |
|
2021 |
|
|
385,000 |
|
|
— |
|
|
— |
|
|
|
99,204 |
|
|
(1 |
) |
— |
|
|
|
484,204 |
|
|||
Willis C. Lee, M.S. |
|
2022 |
|
|
240,000 |
|
|
— |
|
|
— |
|
|
— |
|
|
|
— |
|
|
|
240,000 |
|
|||||
Chief Operating Officer |
|
2021 |
|
|
240,000 |
|
|
|
100,000 |
|
|
— |
|
|
— |
|
|
|
— |
|
|
|
340,000 |
|
||||
Yasushi Nagasaki |
|
2022 |
|
|
250,000 |
|
|
— |
|
|
— |
|
|
— |
|
|
|
— |
|
|
|
250,000 |
|
|||||
Chief Financial Officer |
|
2021 |
|
|
240,000 |
|
|
|
100,000 |
|
(2) |
— |
|
|
— |
|
|
|
— |
|
|
|
340,000 |
|
||||
The compensation of Dr. Niihara and Mr. Lee does not reflect annual performance bonuses contemplated by their respective employment agreements. No specific performance criteria were established for payment of such bonuses for 2022 or 2021, although Mr. Lee was awarded a discretionary bonus in 2021 as shown in the summary compensation table.
60
Outstanding Equity Awards at 2022 Fiscal Year End
The following table sets forth information regarding outstanding equity awards held by our named executive
officers as of December 31, 2022:
Name |
|
Number of Securities |
|
|
Number of Securities |
|
|
Exercise |
|
|
Expiration |
|||
Yutaka Niihara, M.D., MPH |
|
|
315,043 |
|
|
|
— |
|
|
$ |
4.76 |
|
|
5/10/2026 |
|
|
|
500,000 |
|
|
|
— |
|
|
$ |
2.50 |
|
|
8/9/2027 |
Willis C. Lee, M.S. |
|
|
315,043 |
|
|
|
— |
|
|
$ |
4.76 |
|
|
5/10/2026 |
Yasushi Nagasaki |
|
|
315,043 |
|
|
|
— |
|
|
$ |
4.76 |
|
|
5/10/2026 |
Employment Agreements
On April 5, 2011, we entered into employment agreements with Dr. Niihara and Mr. Lee. Each of the Employment Agreements had an initial two-year term, which renews automatically for consecutive one-year periods unless we or the officer provides notice of non-renewal at least 60 days prior to the expiration of the then current term.
Base Salary, Bonus and Other Compensation. Dr. Niihara’s and Mr. Lee’s current base salaries are $385,000 and $240,000 per year, respectively, which will be reviewed at least annually. In addition to the base salary, each officer may be entitled to receive an annual performance bonus based on the officer’s performance. The Employment Agreements provide that the respective officer’s performance will be measured against a set of targets and goals as mutually established by us and the officer. Historically, our board of directors and the Compensation Committee of the board have evaluated each officer’s performance on an overall basis related to our progress on major milestones, without reliance on specific position by position pre-established targets and goals. The officers are also eligible to receive paid vacation and to participate in health and other benefit plans and to be reimbursed for reasonable and necessary business expenses on the same basis as our other employees.
Equity Compensation. The Employment Agreements provide that on December 31 of each calendar year, or as soon as reasonably practicable after such date (each a “Grant Date”), we will grant non-qualified 10-year stock options with a Black-Scholes-Merton value of $100,000 to Dr. Niihara, and $50,000 to Mr. Lee in each case with an exercise price per share equal to the “Fair Market Value” (as such term is defined in our 2011 Stock Incentive Plan) on the applicable Grant Date. The options are to vest as to one-third of the option shares on each of the first three anniversaries of the Grant Date. Any unvested options are to vest immediately upon a change in control (as defined below), termination of the officer’s employment other than a voluntary termination by the officer or our termination of the officer for cause. In the event the officer is terminated for any reason other than cause, death or disability or retirement, each option, to the extent that it is exercisable at the time of such termination, shall remain exercisable for the 90-day period following such termination, but in no event following the expiration of its term. In the event the officer’s employment terminates on account of death, disability or, with respect to any non-qualified stock option, retirement, each option granted that is outstanding and vested as of the date of such termination shall remain exercisable by such officer (or the officer’s legal representatives, heirs or legatees) for the one-year period following such termination, but in no event following the expiration of its term. No such stock option grants were made for either of the years ended December 31, 2022 or 2021.
Severance Compensation. If Dr. Niihara’s or Mr. Lee’s employment is terminated for any reason during the term of his Employment Agreement, other than for cause or without good reason, he will be entitled to receive his or her base salary prorated through the termination date, any expense reimbursement due and owing for reasonable and necessary business expenses, and unpaid vacation benefits (the “Voluntary Termination Benefits”). If Dr. Niihara’s or Mr. Lee’s employment is terminated due to his death or disability during the term of his employment agreement, he will also receive an amount equal to his target annual performance bonus, if any, and in the case of a termination due to disability, six additional months of his base salary to be paid out over a six-month period and payment of COBRA benefits for six months following the termination. If Dr. Niihara’s employment is terminated without cause or he resigns with good reason (but not within two years following a change in control), he will receive the Voluntary Termination Benefits and, subject to his signing a Release of all claims relating to his employment, a severance package equal to one year’s base salary to be paid out over a 12-month period, a pro rata amount of the annual performance bonus for the calendar year in which the termination date occurs based on the achievement of any applicable performance terms or goals for the year, and payment of COBRA benefits for 12 months following the termination. If Mr. Lee’s employment is terminated without cause or he resigns with good reason (but not within two years following a change in control) during the term of his employment agreement, he will receive the Voluntary Termination Benefits and, subject to his signing a Release if all claims relating to his employment, a severance package equal
61
to six months’ base salary to be paid out over a six-month period, an amount equal to half of the targeted annual performance bonus, if any, and payment of COBRA benefits for six months following the termination.
Termination with cause includes a proven act of dishonesty, fraud, embezzlement or misappropriation of company proprietary information; a conviction of, or plea of nolo contendere to, a felony or a crime involving moral turpitude; willful misconduct which cannot be cured on reasonable notice to the officer; or the officer’s habitual failure or refusal to perform his duties if such failure or refusal is not cured within 20 days after receiving written notice thereof from the board of directors. Good reason includes a reduction of more than 10% to the officer’s base salary or other compensation (except as part of a general reduction for all executive employees); a material diminution of the officer’s authority, responsibilities, reporting or job duties (except for any reduction for cause); the company’s material breach of the Employment Agreement; or a relocation of the business requiring the officer to move or drive to work more than 40 miles from the location of our former offices. The officer may terminate the Employment Agreement for good reason if he provides written notice to the Company within 90 days of the event constituting good reason and the Company fails to cure the good reason within 30 days after receiving such notice.
Change of Control. The Employment Agreements will not be terminated upon a “change of control,” which means any merger or reorganization where the holders of the company’s capital stock prior the transaction own fewer than 50% of the shares of capital stock after the transaction, an acquisition of 50% of the voting power of the company’s outstanding securities by another entity, or a transfer of at least 50% of the fair market value of the company’s assets. Upon Dr. Niihara’s termination without cause or for good reason that occurs within two years after a change of control, he will be entitled to receive the Voluntary Termination Benefits and, subject to his signing a Release of all claims relating to his employment, a severance package equal to two years’ base salary to be paid out over a 12-month period, an amount equal to double his targeted annual performance bonus, if any, payment of COBRA benefits for 18 months following the termination, and a one-time cash payment of $3.0 million. Upon Mr. Lee’s termination without cause or for good reason that occurs within two years after a change of control, he will be entitle to receive the Voluntary Termination Benefits and, subject to his signing a Release of all claims relating to his employment, a severance package equal to one year’s base salary to be paid out over a 12-month period, an amount equal to the full-year targeted annual performance bonus, payment of COBRA benefits for 12 months following the termination, and a one-time cash payment of $200,000. In addition, each officer’s unvested equity awards shall vest upon such termination and the officer will have 36 months in which to sell or exercise such awards (subject to expiration of the term of such options). The officer will also be free from all lock-up or other contractual restrictions upon the free sale of shares that are subject to waiver by the Company upon such termination.
Director Compensation
The following is a summary of the compensation of our non-employee directors for 2022:
The following table sets forth information regarding the compensation earned by our non-employee directors for the fiscal year ended December 31, 2022. Our employee directors, Dr. Niihara, and Mr. Lee, are not compensated for their services as directors.
Name |
|
Fees Earned or |
|
|
Option |
|
|
Total |
|
|||
Wei Peu Zen |
|
$ |
100,000 |
|
|
$ |
— |
|
|
$ |
100,000 |
|
Seah H. Lim, M.D., Ph.D (1) |
|
|
25,000 |
|
|
|
— |
|
|
|
25,000 |
|
Ian Zwicker (1) |
|
|
50,000 |
|
|
|
— |
|
|
|
50,000 |
|
Robert Dickey IV (2) |
|
|
59,444 |
|
|
|
— |
|
|
|
59,444 |
|
Jane Pine Wood (2) |
|
|
50,000 |
|
|
|
— |
|
|
|
50,000 |
|
Alfred Lui, M.D. (2) |
|
|
50,000 |
|
|
|
— |
|
|
|
50,000 |
|
Masaharu Osato, M.D. (2) |
|
|
75,000 |
|
|
|
— |
|
|
|
75,000 |
|
Lori Teranishi (2) |
|
|
50,000 |
|
|
|
— |
|
|
|
50,000 |
|
Total |
|
$ |
459,444 |
|
|
$ |
— |
|
|
$ |
459,444 |
|
(1) Mr. Zwicker and Dr. Lim were elected as directors during fiscal year 2022. |
|
|||||||||||
(2) These individuals resigned as directors during fiscal year 2022. |
|
|
|
|
|
|
|
|
|
|||
62
ITEM 12. SECURITY OWNERSHIP OF CERTAIN BENEFICIAL OWNERS AND MANAGEMENT AND RELATED STOCKHOLDER MATTERS
The following table sets forth certain information as of March 15, 2023 with respect to beneficial ownership of our common stock based on issued and outstanding shares of common stock owned by:
Beneficial ownership is determined in accordance with the rules of the SEC. In computing the number of shares beneficially owned by a person and the percentage of ownership of that person, shares of common stock subject to options, warrants and convertible notes held by that person that are currently exercisable or become exercisable within 60 days of March 15, 2023 are deemed outstanding even if they have not actually been exercised. Those shares, however, are not deemed outstanding for the purpose of computing the percentage ownership of any other person.
Unless otherwise indicated, the persons and entities named in the table have sole voting and sole investment power with respect to the shares set forth opposite the stockholder’s name, subject to community property laws, where applicable.
Unless otherwise indicated in the table or footnotes, the address of each 5% or more owner is c/o Emmaus Life Sciences, Inc., 21250 Hawthorne Boulevard, Suite 800, Torrance, California 90503.
63
Name of Beneficial Owner |
|
Title |
|
Amount and |
|
|
Percent of |
|
||
Directors and Executive Officers |
|
|
|
|
|
|
|
|
||
Yutaka Niihara, M.D., M.P.H. |
|
Chairman and Chief Executive Officer |
|
|
20,517,894 |
|
(2) |
|
34.6 |
% |
Willis C. Lee |
|
Director, Chief Operating Officer |
|
|
1,345,861 |
|
(3) |
|
2.6 |
% |
Yasushi Nagasaki |
|
Chief Financial Officer |
|
|
532,145 |
|
(4) |
|
1.0 |
% |
George Sekulich |
|
SVP of Global Commercialization |
|
|
200,147 |
|
(5) |
* |
|
|
Charles Stark |
|
SVP of Clinical Development and Medical Affairs, Clinical, Regulatory |
|
|
328,210 |
|
(6) |
* |
|
|
Seah H. Lim |
|
Director |
|
|
340,000 |
|
(7) |
* |
|
|
Wei Peu Zen |
|
Director |
|
|
2,378,048 |
|
(8) |
|
4.7 |
% |
Ian H. Zwicker |
|
Director |
|
|
100,000 |
|
(9) |
* |
|
|
Officers and Directors as a Group (8 persons) |
|
|
|
|
25,742,305 |
|
(10) |
|
41.8 |
% |
|
|
|
|
|
|
|
|
|
||
5% or More Owners |
|
|
|
|
|
|
|
|
||
Telcon RF Pharmaceutical, Inc. |
|
|
|
|
4,147,491 |
|
(11) |
|
8.1 |
% |
__________ |
|
|
|
|
|
|
|
|
||
* Represents beneficial ownership of less than one percent (1%). |
|
|
|
|
|
|
||||
(1) Based on 50,934,852 shares of common stock issued and outstanding as of March 15, 2023. |
|
|||||||||
(2) Includes 12,047,057 shares of common that are held jointly by Dr. Niihara and Soomi Niihara, his wife. Also includes 63,000 shares held by Soomi Niihara and 92,794 shares owned by Hope International Hospice, Inc., or Hope Hospice. Dr. Niihara is the chief executive officer and a co-director of Hope Hospice and shares voting and investment power over such shares. Also includes 315,043 shares underlying stock options and 8,000,000 shares underlying warrants." Dr. Niihara's address is c/o the Company, 21250 Hawthorne Boulevard, Suite 800, Torrance, CA 90503. |
|
|||||||||
(3) Includes 815,043 shares underlying stock options. |
|
|||||||||
(4) Includes 465,043 shares underlying stock options. |
|
|||||||||
(5) Includes 199,762shares underlying stock options. |
|
|||||||||
(6) Includes 310,028 shares underlying stock options. |
|
|||||||||
(7) Includes 100,000 shares underlying stock options and 240,000 shares issuable upon maturity or prepayment of a promissory note held by Dr. Lim. |
|
|||||||||
(8) Includes 1,270,214 shares owned by Profit Preview International Group Limited, a Hong Kong limited company wholly owned by Mr. Zen. Excludes 521,827 shares owned by Smart Start investments Limited, a Hong Kong corporation and wholly owned subsidiary of Build King Holdings Limited, a Hong Kong stock exchange listed company, of which the Mr. Zen is a director and 9.96% shareholder, and 350,048 shares owned by Wealth Threshold Limited, a British Virgin Islands limited company and wholly owned subsidiary of Wai Kee Holdings Limited, a Hong Kong stock exchange listed company of which Mr. Zen is a director and 31.45% shareholder, as to which shares Mr. Zen disclaims beneficial ownership. |
|
|||||||||
(9) Consists of shares underlying stock options. |
|
|||||||||
(10) Includes 2,40,919 shares underlying stock options, 8,000,000 shares underlying warrants and 240,000 shares issuable upon maturity or prepayment of the promissory note referred to in note 7. |
|
|||||||||
(11) The information regarding Telcon RF Pharmaceutical, Inc. is based solely on its Schedule 13/G filed with the SEC on August 26, 2019. The address for the stockholder is S-Tower 14th Floor 439 Bongunsa-ro, Gangnam-gu, Seoul, South Korea. |
|
|||||||||
ITEM 13. CERTAIN RELATIONSHIPS AND RELATED TRANSACTIONS, AND DIRECTOR INDEPENDENCE
Except as described below in this section, since the beginning of our last fiscal year, there has not been, nor is there currently proposed, there has not been any transaction or series of similar transactions to which we were a party:
64
Loans by Related Persons
In January 2020, we entered into revolving line of credit agreement with Dr. Yutaka Niihara. Under the agreement, at our request from time to time, Dr. Niihara may, but is not obligated to, loan or re-loan to us up to $1,000,000, including $600,000 loaned to us in December 2019. Outstanding amounts under the agreement are due and payable upon demand and bear interest, payable monthly, at a variable annual rate equal to the Prime Rate in effect from time to time plus 3%. In addition to the payment of interest, we agreed to pay Dr. Niihara an amount, which we refer to as a “tax gross-up,” intended to make him whole for federal and state income taxes payable by him with respect to interest paid to him the previous year. The revolving line of credit agreement expired on November 22, 2022 and the Company paid the outstanding principal balance of $400,000 and unpaid interest in December 2022. Refer to Note 12 of the Notes to Financial Statement for more related party information.
The following table sets forth information relating to loans from related parties evidenced by promissory notes payable and convertible promissory notes payable to related persons outstanding at any time during the fiscal year ended December 31, 2022 (amounts in thousands).
Class |
Lender |
|
Interest |
|
Date of |
|
Term of Loan |
|
Principal Amount Outstanding December 31, 2022 |
|
|
Highest |
|
|
Amount of |
|
|
Amount of |
|
||||
Current, Promissory note payable to related parties: |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
Willis Lee(2) |
|
12% |
|
10/29/2020 |
|
Due on Demand |
|
|
100 |
|
|
|
100 |
|
|
|
— |
|
|
|
— |
|
|
Soomi Niihara(1) |
|
12% |
|
12/7/2021 |
|
Due on Demand |
|
|
700 |
|
|
|
700 |
|
|
|
— |
|
|
|
— |
|
|
Soomi Niihara(1) |
|
12% |
|
1/18/2022 |
|
Due on Demand |
|
|
— |
|
|
|
300 |
|
|
|
300 |
|
|
|
32 |
|
|
Yasushi Nagasaki(2) |
|
10% |
|
2/9/2022 |
|
Due on Demand |
|
|
— |
|
|
|
50 |
|
|
|
50 |
|
|
|
4 |
|
|
Hope International Hospice, Inc.(1) |
|
10% |
|
2/9/2022 |
|
Due on Demand |
|
|
350 |
|
|
|
350 |
|
|
|
— |
|
|
|
— |
|
|
Hope International Hospice, Inc.(1) |
|
10% |
|
2/15/2022 |
|
Due on Demand |
|
|
210 |
|
|
|
210 |
|
|
|
— |
|
|
|
— |
|
|
Soomi Niihara(1) |
|
10% |
|
2/15/2022 |
|
Due on Demand |
|
|
100 |
|
|
|
100 |
|
|
|
— |
|
|
|
— |
|
|
George Sekulich(2) |
|
10% |
|
2/16/2022 |
|
Due on Demand |
|
|
— |
|
|
|
26 |
|
|
|
26 |
|
|
|
2 |
|
|
Soomi Niihara(1) |
|
10% |
|
3/7/2022 |
|
Due on Demand |
|
|
— |
|
|
|
200 |
|
|
|
200 |
|
|
|
15 |
|
The proceeds of the above loans were used working capital and general corporate purposes.
Policy for Approval of Related Party Transactions
The Audit Committee of our Board of Directors is responsible for reviewing and approving all related party transactions.
ITEM 14. PRINCIPAL ACCOUNTING FEES AND SERVICES
The following table presents all fees, including reimbursements for expenses, billed for professional services rendered by Baker Tilly US, LLP, our independent registered public accounting firm, for the years ended December 31, 2022 and 2021 (in thousands):
|
|
2022 |
|
|
2021 |
|
||
Audit Fees |
|
$ |
249 |
|
|
$ |
218 |
|
Audit–Related Fees |
|
|
— |
|
|
|
— |
|
Tax Fees |
|
|
— |
|
|
|
— |
|
All Other Fees |
|
|
— |
|
|
|
— |
|
Total |
|
$ |
249 |
|
|
$ |
218 |
|
65
The Audit Committee has adopted a formal policy on auditor independence requiring the advance approval by the Audit Committee of all audit and non-audit services provided by our independent registered public accounting firm. In determining whether to approve any services by our independent registered public accounting firm, the Audit Committee reviews the scope of and estimated fees for the services and considers whether the proposed services may adversely affect the firm’s independence. On an annual basis, our management reports to the Audit Committee all audit services performed during the previous 12 months and all fees billed by our independent registered public accounting firm for such services.
In fiscal 2022 and 2021, all audit services and the corresponding fees were approved by the Audit Committee.
66
PART IV
ITEM 15. EXHIBITS AND FINANCIAL STATEMENT SCHEDULES
Exhibit Index
|
|
Incorporated by Reference |
|
|||
Exhibit Number |
Exhibit Description |
Form |
File No. |
Exhibit |
Filing Date |
Filed/ |
3.1 |
10-K |
001-35527 |
3.1 |
January 25, 2021 |
|
|
3.2 |
8-K |
001-35527 |
3.4 |
July 22, 2019 |
|
|
4.1 |
10-K |
001-35527 |
4.1 |
March 31, 2022 |
|
|
4.2+ |
DEF14A |
001-35527 |
Annex B |
October 12, 2021 |
|
|
4.3+ |
Form of Incentive Stock Option Agreement under 2021 Stock Incentive Plan |
S-8 |
001-35527 |
4.2 |
December 30, 2021 |
|
4.4+ |
S-8 |
001-35527 |
4.3 |
December 30, 2021 |
|
|
4.5+ |
Form of Non-Qualified Stock Option Agreement under 2021 Stock Incentive Plan (Non-Director Grantee) |
S-8 |
001-35527 |
4.4 |
December 30, 2021 |
|
4.6 |
10-K |
000-142031 |
4.32 |
April 16, 2018 |
|
|
4.7 |
10-Q |
000-142031 |
4.1 |
May 15, 2018 |
|
|
4.8+ |
Emmaus Life Sciences, Inc. Amended and Restated 2011 Equity Incentive Plan. |
DEF14A |
000-53072 |
Annex A |
September 19, 2014 |
|
4.9+
|
8-K |
000-142031 |
10.3a |
May 4, 2011 |
|
|
4.10+ |
Form of Incentive Stock Option Agreement (Time-Based Vesting) under 2011 Equity Incentive Plan. |
8-K |
000-142031 |
10.3b |
May 4, 2011 |
|
67
|
|
Incorporated by Reference |
|
|||
Exhibit Number |
Exhibit Description |
Form |
File No. |
Exhibit |
Filing Date |
Filed/ |
4.11+ |
8-K |
000-142031 |
10.3c |
May 4, 2011 |
|
|
4.12+
|
Form of Non-Qualified Stock Option Agreement (Time-Based Vesting) under 2011 Equity Incentive Plan. |
8-K |
000-142031 |
10.3d |
May 4, 2011 |
|
4.13+ |
8-K |
000-142031 |
10.3e |
May 4, 2011 |
|
|
4.14+ |
Form of Restricted Stock Agreement (Time-Based Vesting) under 2011 Equity Incentive Plan. |
8-K |
000-142031 |
10.3f |
May 4, 2011 |
|
4.15 |
10-K |
001-35527 |
10.14 |
December 11, 2018 |
|
|
4.16 |
Form of Second Amended and Restated Common Stock Purchase Warrant. |
8-K |
001-35527 |
4.2 |
February 27, 2020 |
|
4.17 |
10-K |
001-35527 |
4.24 |
May 4, 2021 |
|
|
4.18 |
10-K |
001-35527 |
4.25 |
May 4, 2021 |
|
|
4.19 |
8-K |
001-35527 |
10.1 |
September 24, 2020 |
|
|
4.20 |
10-K |
001-35527 |
4.27 |
May 4, 2021 |
|
|
10.1 |
10-Q |
001-35527 |
10.7 |
November 13, 2019 |
|
|
10.2+ |
8-K |
000-142031 |
10.12 |
May 4, 2011 |
|
|
68
|
|
Incorporated by Reference |
|
|||
Exhibit Number |
Exhibit Description |
Form |
File No. |
Exhibit |
Filing Date |
Filed/ |
10.3+ |
Executive Employment Agreement dated as of April 5, 2011 between Emmaus Medical, Inc. and Willis Lee. |
8-K |
000-142031 |
10.13 |
May 4, 2011 |
|
10.4+ |
8-K |
000-142031 |
10.20 |
May 4, 2011 |
|
|
10.5 |
Letter of Intent by and between Ajinomoto Aminoscience LLC and Emmaus Medical, Inc. |
8-K/A |
000-142031 |
10.24 |
July 5, 2011 |
|
10.6 |
10-K |
001-35527 |
10.23(F) |
March 31, 2015 |
|
|
10.7 |
10-K |
000-142031 |
10.24a |
March 21, 2019 |
|
|
10.8 |
10-K |
000-142031 |
10.24b |
March 21, 2019 |
|
|
10.9 |
10-K |
001-35527 |
10.23 |
January 25, 2021 |
|
|
10.10
|
10-Q |
000-142031 |
10.3 |
November 14, 2017 |
|
|
10.11 |
10-K |
001-35527 |
10.25 |
January 25, 2021 |
|
|
69
|
|
Incorporated by Reference |
|
|||
Exhibit Number |
Exhibit Description |
Form |
File No. |
Exhibit |
Filing Date |
Filed/ |
10.12 |
10-K |
001-35527 |
10.26 |
January 25, 2021 |
|
|
10.13 |
10-K |
001-35527 |
10.27 |
January 25, 2021 |
|
|
10.14 |
10-K |
001-35527 |
10.28 |
January 25, 2021 |
|
|
10.15 |
10-K |
001-35527 |
10.29 |
January 25, 2021 |
|
|
10.16 |
10-K |
001-35527 |
10.35 |
January 25, 2021 |
|
|
10.17 |
Loan Agreement Dated October 28, 2020 Between Emmaus Life Sciences, Inc. and EJ Holdings, Inc. |
8-K |
001-35527 |
10.1 |
November 13, 2020 |
|
10.18 |
10-K |
001-35527 |
10.21 |
March 31, 2022 |
|
|
10.19 |
License Agreement between Kainos Medicine, Inc. and Emmaus Life Sciences, Inc. |
10-K |
001-35527 |
10.22 |
March 31, 2022 |
|
10.20 |
Promissory Note dated April 24, 2021 issued by registrant to Eastwind, Ltd. |
10-Q |
001-35527 |
10.1 |
September 1, 2021 |
|
70
|
|
Incorporated by Reference |
|
|||
Exhibit Number |
Exhibit Description |
Form |
File No. |
Exhibit |
Filing Date |
Filed/ |
10.21 |
Promissory Note dated February 17, 2021 issued by registrant to Shigeru Matsuda. |
10-Q |
001-35527 |
10.2 |
September 1, 2021 |
|
10.22 |
Promissory Note dated May 26, 2021 issued by registrant to Shigeru Matsuda. |
10-Q |
001-35527 |
10.2 |
September 1, 2021 |
|
10.23 |
Promissory Note dated December 7, 2021 issued by registrant to Soomi Niihara. |
10-K |
001-35527 |
10.26 |
March 31, 2022 |
|
10.24+ |
10-K
|
001-35527 |
10.37 |
January 25, 2021 |
|
|
10.25 |
10-K |
001-35527 |
10.37 |
May 4, 2021 |
|
|
10.26 |
10-K |
001-35527 |
10.38 |
May 4, 2021 |
|
|
10.27 |
8-K |
001-35527 |
10.1 |
February 16, 2021 |
|
|
10.28 |
8-K |
001-35527 |
10.2 |
February 16, 2021 |
|
|
10.29 |
8-K |
001-35527 |
10.1 |
February 22, 2021 |
|
|
10.30 |
Guaranty dated December 9, 2020 by Emmaus Life Sciences, Inc. in favor or Prestige Capital, Inc. |
8-K |
001-35527 |
10.2 |
February 22, 2021 |
|
71
72
|
|
Incorporated by Reference |
|
|||
Exhibit Number |
Exhibit Description |
Form |
File No. |
Exhibit |
Filing Date |
Filed/ |
23.1 |
Consent of Independent Registered Public Accounting Firm Baker Tilly US, LLP. |
|
|
|
|
* |
31.1 |
|
|
|
|
* |
|
31.2 |
|
|
|
|
* |
|
32.1 |
|
|
|
|
* |
|
101.INS |
Inline XBRL Instance Document – the instance document does not appear in the Interactive Data File because XBRL tags are embedded within the Inline XBRL document |
|
|
|
|
|
101.SCH |
Inline XBRL Taxonomy Extension Schema Document |
|
|
|
|
|
101.CAL |
Inline XBRL Taxonomy Extension Calculation Linkbase Document |
|
|
|
|
|
101.DEF |
Inline XBRL Taxonomy Extension Definition Linkbase Document |
|
|
|
|
|
101.LAB |
Inline XBRL Taxonomy Extension Label Linkbase Document |
|
|
|
|
|
101.PRE |
Inline XBRL Taxonomy Extension Presentation Linkbase Document |
|
|
|
|
|
104 |
Cover Page Interactive Data File (embedded within the Inline XBRL document) |
|
|
|
|
|
__________________________________
+ Management contract or compensatory plan, contract or arrangement
* Filed herewith.
73
SIGNATURES
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the Registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized, in the City of Torrance, California.
Emmaus Life Sciences, Inc. |
||
|
||
By: |
|
/s/ Yutaka Niihara |
|
|
Yutaka Niihara, M.D., M.P.H. |
Title: |
|
Chairman and Chief Executive Officer |
Date |
|
March 31, 2023 |
|
|
|
By: |
|
/s/ Yasushi Nagasaki |
|
|
Yasushi Nagasaki |
Title: |
|
Chief Financial Officer (Principal Financial and Accounting Officer) |
Date |
|
March 31, 2023 |
74
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed below by the following persons on behalf of the registrant and in the capacities and on the dates indicated.
POWER OF ATTORNEY
Each person whose signature appears below constitutes and appoints Yutaka Niihara, M.D., M.P.H. and Yasushi Nagasaki, jointly and severally, as his or her attorneys-in-fact, each with the power of substitution, for him or her in any and all capacities, to sign any amendments to this Annual Report on Form 10-K, and to file the same, with exhibits thereto and other documents in connection therewith, with the Securities and Exchange Commission, hereby ratifying and confirming all that each of said attorneys-in-fact, or his substitute or substitutes, may do or cause to be done by virtue hereof.
By: |
|
/s/ Willis Lee |
|
|
Willis Lee |
Title: |
|
Director and Chief Operating Officer |
Date |
|
March 31, 2023 |
|
|
|
By: |
|
/s/ Wei Peu Zen |
|
|
Wei Peu Zen |
Title: |
|
Director |
Date |
|
March 31, 2023 |
|
|
|
By: |
|
/s/ Ian Zwicker |
|
|
Ian Zwicker |
Title: |
|
Director |
Date |
|
March 31, 2023 |
|
|
|
By: |
|
/s/ Seah Lim |
|
|
Shea Lim |
Title: |
|
Director |
Date |
|
March 31, 2023 |
|
|
|
75
INDEX TO FINANCIAL STATEMENTS
EMMAUS LIFE SCIENCES, INC.
INDEX TO CONSOLIDATED FINANCIAL STATEMENTS
F-1
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
To the Stockholders and the Board of Directors of Emmaus Life Sciences, Inc.
Opinion on the Financial Statements
We have audited the accompanying consolidated balance sheets of Emmaus Life Sciences, Inc. and its subsidiaries (the “Company”) as of December 31, 2022 and 2021, the related consolidated statements of operations and comprehensive loss, changes in stockholders' deficit, and cash flows, for the years then ended, and the related notes to the consolidated financial statements (collectively, the “financial statements”). In our opinion the consolidated financial statements present fairly, in all material respects, the financial position of the Company at December 31, 2022 and 2021, and the results of its operations and its cash flows for the years then ended, in conformity with accounting principles generally accepted in the United States of America.
Going Concern Uncertainty
The accompanying consolidated financial statements have been prepared assuming that the Company will continue as a going concern. As discussed in Note 2 to the consolidated financial statements, the Company has incurred recurring operating losses and its current liabilities exceed its current assets. These conditions raise substantial doubt about the Company’s ability to continue as a going concern. Management’s plans in regard to these matters are also described in Note 2. The consolidated financial statements do not include any adjustments that might result from the outcome of this uncertainty.
Basis for Opinion
These consolidated financial statements are the responsibility of the Company's management. Our responsibility is to express an opinion on the Company's consolidated financial statements based on our audits. We are a public accounting firm registered with the Public Company Accounting Oversight Board (United States) (“PCAOB”) and are required to be independent with respect to the Company in accordance with U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audits in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audits to obtain reasonable assurance about whether the consolidated financial statements are free of material misstatement, whether due to error or fraud. The Company is not required to have, nor were we engaged to perform, an audit of its internal control over financial reporting. As part of our audits we are required to obtain an understanding of internal control over financial reporting but not for the purpose of expressing an opinion on the effectiveness of the Company’s internal control over financial reporting. Accordingly, we express no such opinion.
Our audits included performing procedures to assess the risks of material misstatement of the consolidated financial statements, whether due to error or fraud, and performing procedures that respond to those risks. Such procedures included examining, on a test basis, evidence regarding the amounts and disclosures in the consolidated financial statements. Our audits also included evaluating the accounting principles used and significant estimates made by management, as well as evaluating the overall presentation of the consolidated financial statements. We believe that our audits provide a reasonable basis for our opinion.
F-2
Critical Audit Matters
The critical audit matters communicated below are matters arising from the current-period audit of the consolidated financial statements that were communicated or required to be communicated to the Company’s Audit Committee and that: (1) relate to accounts or disclosures that are material to the consolidated financial statements and (2) involved our especially challenging, subjective, or complex judgments. The communication of critical audit matters does not alter in any way our opinion on the consolidated financial statements, taken as a whole, and we are not, by communicating the critical audit matters below, providing separate opinions on the critical audit matters or on the accounts or disclosures to which they relate.
REVENUE RECOGNITION - VARIABLE CONSIDERATION
Critical Audit Matter Description
As described in Note 2 to the consolidated financial statements, the Company records revenue at the transaction price, net of estimates for variable consideration consisting primarily of chargebacks, discounts, and returns, which are established at the time of sales. The Company recorded sales deductions of $8.3 million during the year ended of December 31, 2022. Actual amounts of consideration ultimately received may differ from estimates. If actual results vary materially from estimates, the Company will adjust these estimates, which will affect net sales of the products and results from operations in the period such estimates are adjusted.
We identified the determination of variable consideration as a critical audit matter. Significant judgment is exercised by the Company in estimating variable consideration when determining the amount of revenue to recognize. Given these factors, the related audit effort in evaluating management’s judgments in determining the amount of variable consideration used to determine the transaction price was extensive and required a high degree of auditor judgment.
How We Addressed the Matter in Our Audit
The primary procedures we performed to address this critical audit matter included:
F-3
INVESTMENT IN CONVERTIBLE BOND AND CONVERSION FEATURE OF CONVERTIBLE NOTES PAYABLE – DETERMINATION OF FAIR VALUE
Critical Audit Matter Description
As described in Note 5 to the consolidated financial statements, the Company purchased a convertible bond and elected the fair value accounting option. The fair value of the convertible bond was $20 million as of December 31, 2022. The fair value was determined using a Lattice pricing model and the change in fair value was recorded as part of other comprehensive loss.
As described in Note 7 to the consolidated financial statements, the Company issued convertible notes payable resulting in liability treatment of the conversion feature. The fair value of the conversion feature was $3.2 million as of December 31, 2022. The fair value was determined using a Lattice pricing model and the change in fair value was recorded as part of net loss.
We identified the determination of the fair value using the binomial lattice model as a critical audit matter. Significant judgment is exercised by the Company in determining the fair value of the convertible bond and the conversion feature of the convertible notes payable. Given these factors, the related audit effort in evaluating management’s judgments in determining the fair value of the convertible bond and the conversion feature of the convertible notes payable was complex and required a high degree of auditor judgment.
How We Addressed the Matter in Our Audit
The primary procedures we performed to address this critical audit matter included:
/s/
We have served as the Company's auditor since 2020.
March 31, 2023
F-4
Emmaus Life Sciences, Inc.
Consolidated Balance Sheets
(In thousands, except share and per share amounts)
|
|
As of |
|
|||||
|
|
December 31, 2022 |
|
|
December 31, 2021 |
|
||
ASSETS |
|
|
|
|
|
|
||
CURRENT ASSETS |
|
|
|
|
|
|
||
Cash and cash equivalents |
|
$ |
|
|
$ |
|
||
Accounts receivable, net |
|
|
|
|
|
|
||
Inventories, net |
|
|
|
|
|
|
||
Prepaid expenses and other current assets |
|
|
|
|
|
|
||
Total current assets |
|
|
|
|
|
|
||
Property and equipment, net |
|
|
|
|
|
|
||
Equity method investment |
|
|
|
|
|
|
||
Right of use assets |
|
|
|
|
|
|
||
Investment in convertible bond |
|
|
|
|
|
|
||
Other assets |
|
|
|
|
|
|
||
Total assets |
|
$ |
|
|
$ |
|
||
LIABILITIES AND STOCKHOLDERS’ DEFICIT |
|
|
|
|
|
|
||
CURRENT LIABILITIES |
|
|
|
|
|
|
||
Accounts payable and accrued expenses |
|
$ |
|
|
$ |
|
||
Operating lease liabilities, current portion |
|
|
|
|
|
|
||
Conversion feature derivative, notes payable |
|
|
|
|
|
|
||
Other current liabilities |
|
|
|
|
|
|
||
Revolving line of credit from related party |
|
|
— |
|
|
|
|
|
Warrant derivative liabilities |
|
|
|
|
|
|
||
Notes payable, current portion, net of discount |
|
|
|
|
|
|
||
Notes payable to related parties |
|
|
|
|
|
|
||
Convertible notes payable, net of discount |
|
|
|
|
|
|
||
Total current liabilities |
|
|
|
|
|
|
||
Operating lease liabilities, less current portion |
|
|
|
|
|
|
||
Other long-term liabilities |
|
|
|
|
|
|
||
Notes payable, less current portion |
|
|
|
|
|
|
||
Notes payable to related parties, net |
|
|
|
|
|
— |
|
|
Convertible notes payable |
|
|
— |
|
|
|
|
|
Total liabilities |
|
|
|
|
|
|
||
STOCKHOLDERS’ DEFICIT |
|
|
|
|
|
|
||
Preferred stock, par value $ |
|
|
|
|
|
|
||
Common stock, par value $ |
|
|
|
|
|
|
||
Additional paid-in capital |
|
|
|
|
|
|
||
Accumulated other comprehensive loss |
|
|
( |
) |
|
|
) |
|
Accumulated deficit |
|
|
( |
) |
|
|
( |
) |
Total stockholders’ deficit |
|
|
( | ) |
|
|
( |
) |
Total liabilities & stockholders’ deficit |
|
$ |
|
|
$ |
|
||
The accompanying notes are an integral part of these consolidated financial statements.
F-5
Emmaus Life Sciences, Inc.
Consolidated Statements of Operations and Comprehensive Loss
(In thousands, except share and per share amounts)
|
|
Years Ended December 31, |
|
|||||
|
|
2022 |
|
|
2021 |
|
||
REVENUES, NET |
|
$ |
|
|
$ |
|
||
COST OF GOODS SOLD |
|
|
|
|
|
|
||
GROSS PROFIT |
|
|
|
|
|
|
||
OPERATING EXPENSES |
|
|
|
|
|
|
||
Research and development |
|
|
|
|
|
|
||
Selling |
|
|
|
|
|
|
||
General and administrative |
|
|
|
|
|
|
||
Total operating expenses |
|
|
|
|
|
|
||
LOSS FROM OPERATIONS |
|
|
( | ) |
|
|
( | ) |
OTHER INCOME (EXPENSE) |
|
|
|
|
|
|
||
Loss on debt extinguishment |
|
|
( |
) |
|
|
( |
) |
Change in fair value of warrant derivative liabilities |
|
|
|
|
|
( |
) |
|
Change in fair value of conversion feature derivative, notes payable |
|
|
|
|
|
( |
) |
|
Loss on investment in convertible bond |
|
|
( |
) |
|
|
— |
|
Net loss on equity method investment |
|
|
( |
) |
|
|
( |
) |
Foreign exchange loss |
|
|
( |
) |
|
|
( |
) |
Interest and other income |
|
|
|
|
|
|
||
Interest expense |
|
|
( |
) |
|
|
( |
) |
Total other expense |
|
|
( |
) |
|
|
( |
) |
LOSS BEFORE INCOME TAXES |
|
|
( |
) |
|
|
( |
) |
Income tax provision |
|
|
|
|
|
|
||
NET LOSS |
|
|
( |
) |
|
|
( |
) |
|
|
|
|
|
|
|
||
COMPONENTS OF OTHER COMPREHENSIVE LOSS |
|
|
|
|
|
|
||
Unrealized loss on debt securities available for sale (net of tax) |
|
|
( |
) |
|
|
( |
) |
Reclassification adjustment for loss included in net income |
|
|
|
|
|
— |
|
|
Foreign currency translation adjustments |
|
|
|
|
|
|
||
Other comprehensive loss |
|
|
( |
) |
|
|
( |
) |
COMPREHENSIVE LOSS |
|
$ |
( |
) |
|
$ |
( |
) |
NET LOSS PER COMMON SHARE - BASIC AND DILUTED |
|
$ |
( |
) |
|
$ |
( |
) |
WEIGHTED-AVERAGE COMMON SHARES OUTSTANDING |
|
|
|
|
|
|
||
The accompanying notes are an integral part of these consolidated financial statements.
F-6
Emmaus Life Sciences, Inc.
Consolidated Statements of changes IN stockholders’ deficit
(In thousands, except share and per share amounts)
|
Common stock |
|
|
Additional paid-in |
|
|
Accumulated other comprehensive |
|
|
Accumulated |
|
|
Total stockholders' |
|
|||||||||
|
Shares |
|
|
Amount |
|
|
capital |
|
|
loss |
|
|
deficit |
|
|
deficit |
|
||||||
Balance, January 1, 2021 |
|
|
|
$ |
|
|
$ |
|
|
$ |
|
|
$ |
( |
) |
|
$ |
( |
) |
||||
Fair value of warrants including down-round protection adjustments |
|
— |
|
|
|
— |
|
|
|
|
|
|
— |
|
|
|
( |
) |
|
|
— |
|
|
Common stock issued for services |
|
|
|
|
— |
|
|
|
|
|
|
— |
|
|
|
— |
|
|
|
|
|||
Share-based compensation |
|
— |
|
|
|
— |
|
|
|
|
|
|
— |
|
|
|
— |
|
|
|
|
||
Unrealized loss on debt securities available for sale (net of tax) |
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
( |
) |
|
|
— |
|
|
|
( |
) |
Foreign currency translation effect |
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
|
|
|
— |
|
|
|
|
||
Net loss |
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
( |
) |
|
|
( |
) |
Balance, December 31, 2021 |
|
|
|
$ |
|
|
$ |
|
|
$ |
( |
) |
|
$ |
( |
) |
|
$ |
( | ) |
|||
Reclassification of warrants from liability to equity |
|
— |
|
|
|
— |
|
|
|
|
|
|
— |
|
|
|
— |
|
|
|
|
||
Fair value of warrants including down-round protection adjustments |
|
— |
|
|
|
— |
|
|
|
|
|
|
— |
|
|
|
( |
) |
|
|
— |
|
|
Common stock issued for services |
|
|
|
|
|
|
|
|
|
|
— |
|
|
|
— |
|
|
|
|
||||
Share-based compensation |
|
— |
|
|
|
— |
|
|
|
|
|
|
— |
|
|
|
— |
|
|
|
|
||
Unrealized loss on debt securities available for sale (net of tax) |
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
( |
) |
|
|
— |
|
|
|
( |
) |
Reclassification adjustment for loss included in net income |
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
|
|
|
— |
|
|
|
|
||
Foreign currency translation effect |
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
|
|
|
— |
|
|
|
|
||
Net loss |
|
|
|
|
|
|
|
|
|
|
|
|
|
( |
) |
|
|
( |
) |
||||
Balance, December 31, 2022 |
|
|
|
$ |
|
|
$ |
|
|
$ |
( | ) |
|
$ |
( |
) |
|
$ |
( | ) |
|||
The accompanying notes are an integral part of these consolidated financial statements.
F-7
Emmaus Life Sciences, Inc.
Consolidated Statements of Cash Flows
(In thousands)
|
|
Years Ended December 31, |
|
|||||
|
|
2022 |
|
|
2021 |
|
||
CASH FLOWS FROM OPERATING ACTIVITIES |
|
|
|
|
|
|
||
Net loss |
|
$ |
( |
) |
|
$ |
( |
) |
Adjustments to reconcile net loss to net cash flows used in operating activities |
|
|
|
|
|
|
||
Depreciation and amortization |
|
|
|
|
|
|
||
Inventory reserve |
|
|
|
|
|
|
||
Amortization of discount of notes payable and convertible notes payable |
|
|
|
|
|
|
||
Foreign exchange adjustments |
|
|
|
|
|
|
||
Net loss on investment in convertible bond |
|
|
|
|
— |
|
||
Loss on equity method investment |
|
|
|
|
|
|
||
Loss on debt extinguishment |
|
|
|
|
|
|
||
Loss (Gain) on disposal of property and equipment |
|
|
|
|
|
( |
) |
|
Loss on leased assets |
|
|
|
|
|
— |
|
|
Share-based compensation |
|
|
|
|
|
|
||
Shares issued for services |
|
|
|
|
|
|
||
Change in fair value of warrant derivative liabilities |
|
|
( |
) |
|
|
|
|
Change in fair value of conversion feature derivative, notes payable |
|
|
( |
) |
|
|
|
|
Changes in fair value of embedded derivative, note payable from related party |
|
|
( |
) |
|
|
— |
|
Net changes in operating assets and liabilities |
|
|
|
|
|
|
||
Accounts receivable |
|
|
|
|
|
( |
) |
|
Inventories |
|
|
|
|
|
|
||
Prepaid expenses and other current assets |
|
|
( |
) |
|
|
|
|
Other non-current assets |
|
|
|
|
|
|
||
Income tax receivable and payable |
|
|
|
|
|
( |
) |
|
Accounts payable and accrued expenses |
|
|
|
|
|
|
||
Other current liabilities |
|
|
( |
) |
|
|
|
|
Other long-term liabilities |
|
|
( |
) |
|
|
( |
) |
Net cash flows used in operating activities |
|
|
( |
) |
|
|
( |
) |
CASH FLOWS FROM INVESTING ACTIVITIES |
|
|
|
|
|
|
||
Proceeds from sale of convertible bond |
|
|
|
|
|
— |
|
|
Purchases of property and equipment |
|
|
( |
) |
|
|
( |
) |
Loan to equity method investee |
|
|
( |
) |
|
|
( |
) |
Net cash flows used in investing activities |
|
|
( |
) |
|
|
( |
) |
CASH FLOWS FROM FINANCING ACTIVITIES |
|
|
|
|
|
|
||
Proceeds from notes payable issued, net of issuance cost |
|
|
|
|
|
— |
|
|
Proceeds from notes payable issued, net of issuance cost, related party |
|
|
|
|
|
|
||
Proceeds from convertible notes payable issued, net of issuance cost and discount |
|
|
— |
|
|
|
|
|
Payments of notes payable |
|
|
( |
) |
|
|
( |
) |
Payments of notes payable, related party |
|
|
( |
) |
|
|
( |
) |
Payments of convertible notes |
|
|
( |
) |
|
|
( |
) |
Net cash flows provided by financing activities |
|
|
|
|
|
|
||
Effect of exchange rate changes on cash |
|
|
( |
) |
|
|
|
|
Net decrease in cash, cash equivalents and restricted cash |
|
|
( |
) |
|
|
( |
) |
Cash, cash equivalents and restricted cash, beginning of period |
|
|
|
|
|
|
||
Cash, cash equivalents and restricted cash, end of period |
|
$ |
|
|
$ |
|
||
|
|
|
|
|
|
|
||
SUPPLEMENTAL DISCLOSURES OF CASH FLOW ACTIVITIES |
|
|
|
|
|
|
||
Interest paid |
|
$ |
|
|
$ |
|
||
Income taxes paid |
|
$ |
|
|
$ |
|
||
NON-CASH INVESING AND FINANCING ACTIVITIES |
|
|
|
|
|
|
||
Debt discount due to embedded derivative |
|
$ |
|
|
$ |
|
||
Debt discount due to deferred financing cost |
|
$ |
|
|
$ |
— |
|
|
Debt discount due to warrants |
|
$ |
|
|
$ |
— |
|
|
Note payable extinguished through issuance of related party note payable. |
|
$ |
|
|
$ |
— |
|
|
The accompanying notes are an integral part of these consolidated financial statements.
F-8
Emmaus Life Sciences, Inc.
Notes to consolidated financial statements
NOTE 1—DESCRIPTION OF BUSINESS
Organization—On July 17, 2019 Emmaus Life Sciences, Inc. (formerly, “MYnd Analytics, Inc.” and herein the “Company” or “Emmaus”) completed its merger transaction (the “Merger”) with EMI Holding, Inc., formerly known as Emmaus Life Sciences, Inc. (“EMI Holding”). In the Merger, a wholly owned subsidiary of the Company merged into EMI Holding, with EMI Holding surviving the Merger as a wholly owned subsidiary. Immediately after completion of the Merger, the Company changed its name to “Emmaus Life Sciences, Inc.”
The Merger was treated as a reverse recapitalization under the acquisition method of accounting in accordance with accounting principles generally accepted in the U.S. (“GAAP”) For accounting purposes, EMI Holding was considered to have acquired the Company.
In connection with and prior to the Merger, the Company contributed and transferred to Telemynd, Inc. (“Telemynd”), a newly formed, subsidiary of the Company, all or substantially all of the Company’s historical business, assets and liabilities and the Company’s board of directors declared a stock dividend of share of the Telemynd common stock held by the Company for each outstanding share of Company common stock after giving effect to a
As a result of the spin-off and the Merger, the Company’s ongoing business became EMI Holding’s business, which is that of a commercial-stage biopharmaceutical company focused on the development, marketing and sale of innovative treatments and therapies, including those in the rare and orphan disease categories.
References herein to the “Company” or “Emmaus” means Emmaus Life Sciences, Inc. and its direct and direct subsidiaries.
Nature of Business—The Company is a commercial-stage biopharmaceutical company engaged in the discovery, development, marketing and sales of innovative treatments and therapies, primarily for rare and orphan diseases. The Company’s lead product Endari® (prescription grade L-glutamine oral powder) is approved by the U.S. Food and Drug Administration, or FDA, to reduce the acute complications of sickle cell disease (“SCD”) in adult and pediatric patients five years of age and older. Endari® has received Orphan Drug designation from the FDA and Orphan Medicinal designation from the European Commission, which designations generally afford marketing exclusivity for Endari® for a
Endari® is marketed and sold by the internal commercial sales team. Endari® is reimbursable by the Centers for Medicare and Medicaid Services, and every state provides coverage for Endari® for outpatient prescriptions to all eligible Medicaid enrollees within their state Medicaid programs. Endari® is also reimbursable by many commercial payors. The Company has agreements in place with the nation’s leading distributors, as well as physician group purchasing organizations and pharmacy benefits managers, making Endari® available at selected retail and specialty pharmacies nationwide.
NOTE 2—SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES
Basis of presentation—The accompanying consolidated financial statements have been prepared in accordance with GAAP codified in the Accounting Standards Codification (“ASC”) and Accounting Standards Updates (“ASU”) of the Financial Accounting Standards Board (“FASB”).
Going concern— The accompanying consolidated financial statements have been prepared on the basis that the Company will continue as a going concern. The Company incurred a net loss of $
F-9
Principles of consolidation—The consolidated financial statements include the accounts of the Company and EMI Holding subsidiary and EMI Holding’s wholly‑owned subsidiary, Emmaus Medical Inc., and Emmaus Medical, Inc’s wholly‑owned subsidiaries. All significant intercompany transactions have been eliminated.
Estimates—Financial statements prepared in accordance with GAAP require management to make estimates and assumptions that affect the reported amounts of assets and liabilities at the date of the financial statements and the reported amounts of revenues and expenses during the reporting period. Significant estimates made by management include those relating to revenue recognition on product sales, the estimated useful lives of equipment, impairment of assets, the variables used to calculate the valuation of conversion features, stock options and warrants, and estimated accruals on an ongoing basis. The Company bases its estimates on historical experience and on various other assumptions that management believes to be reasonable under the circumstances. Actual results could differ from those estimates under different assumptions or conditions. To the extent there are material differences between these estimates and actual results, the Company’s financial statements will be affected.
Revenue recognition— The Company realizes net revenues primarily from sales of Endari® to distributors and specialty pharmacy providers. Distributors resell Endari® to other pharmacy and specialty pharmacy providers, health care providers, hospitals, and clinics. In addition to agreements with these distributors, the Company has contractual arrangements with specialty pharmacy providers, in-office dispensing providers, physician group purchasing organizations, pharmacy benefits managers and government entities that provide for government-mandated or privately negotiated rebates, chargebacks and discounts with respect to the purchase of Endari®. These various discounts, rebates, and chargebacks are referred to as “variable consideration.” Revenue from product sales is recorded net of variable consideration.
Under ASC 606 Revenue from Contracts with Customers, the Company recognizes revenue when its customers obtain control of the Company's product, which typically occurs on delivery. Revenue is recognized in an amount that reflects the consideration that the Company expects to receive in exchange for the product, or transaction price. To determine revenue recognition for contracts with customers within the scope of ASC 606, the Company performs the following 5 steps: (i) identify the contract(s) with a customer; (ii) identify the performance obligations in the contract; (iii) determine the transaction price; (iv) allocate the transaction price to the Company’s performance obligations in the contract; and (v) recognize revenue when (or as) the Company satisfies the relevant performance obligations.
Revenue from product sales is recorded at the transaction price, net of estimates for variable consideration consisting of sales discounts, returns, government rebates, chargebacks and commercial discounts. Variable consideration is estimated using the expected-value amount method, which is the sum of probability-weighted amounts in a range of possible transaction prices. Actual variable consideration may differ from the Company's estimates. If actual results vary from the Company's estimates, the Company adjusts the variable consideration in the period such variances become known, which would affect net revenues in that period. The following are our significant categories of variable consideration:
Sales Discounts: The Company provides its customers prompt payment discounts and from time to time offers additional discounts for bulk orders that are recorded as a reduction of revenues in the period the revenues are recognized.
Product Returns: The Company offers distributors a right to return product purchased principally based upon (i) overstocks, (ii) inactive product or non-moving product due to market conditions, and (iii) expired products. Product return allowances are estimated and recorded at the time of sale.
Government Rebates: The Company is subject to discount obligations under state Medicaid programs and the Medicare Part D prescription drug coverage gap program. Management estimates Medicaid and Medicare Part D prescription drug coverage gap rebates based upon a range of possible outcomes that are probability-weighted for the estimated payor mix. These reserves are recorded in the same period the related revenues are recognized, resulting in a reduction of product revenues and the establishment of a current liability that is included as an accounts payable and accrued expenses in the consolidated balance sheets. The liability for these rebates consists primarily of estimates of claims expected to be received in future periods related to recognized revenues.
Chargebacks and Discounts: Chargebacks for fees and discounts represent the estimated obligations resulting from contractual commitments to sell products to certain specialty pharmacy providers, in-office dispensing providers, group purchasing organizations, and government entities at prices lower than the list prices charged to distributors. The distributors
F-10
charge the Company for the difference between what they pay for the products and the Company’s contracted selling price to these specialty pharmacy providers, in-office dispensing providers, group purchasing organizations, and government entities. In addition, the Company has contractual agreements with pharmacy benefit managers who charge us for rebates and administrative fee in connection with the utilization of product. These reserves are established in the same period that the related revenues are recognized, resulting in a reduction of revenues. Chargeback amounts are generally determined at the time of resale of products by the distributors.
Leases — In accordance with ASC 842 Leases, the Company determines whether an arrangement is a lease at inception. For leases where the Company is the lessee, right-of-use assets and operating lease liabilities are recognized based on the present value of remaining lease payments over the lease term. When the Company’s leases do not provide an implicit rate, the Company uses an estimated incremental borrowing rate based on the information available at lease commencement date in determining the present value of lease payments. Operating lease expense is recognized on a straight-line basis over the lease term. Variable lease costs such as common area costs and other operating costs are expensed as incurred. For all lease agreements, lease and non-lease components are combined. No right-of-use asset and related lease liability are recorded for leases with an initial term of 12 months or less.
Cash and cash equivalents—Cash and cash equivalents include short‑term securities, if any, with original maturities of less than ninety days. The Company maintains its cash and cash equivalents at insured financial institutions, the balances of which may, at times, exceed federally insured limits. Management believes that the risk of loss due to uninsured deposit is minimal.
Accounts receivable— Accounts receivables are primarily attributable to product sales to customers. The Company makes judgements as to its ability to collect outstanding receivables and provides an allowance for receivables if and when collection becomes doubtful. Provisions are made based upon a specific review of all significant outstanding invoices and the quality and age of those invoices. The Company believes the credit risks associated with its customers are not significant.
Factoring accounts receivable— Emmaus Medical, Inc., or Emmaus Medical, the Company’s indirect wholly owned subsidiary, entered into a purchase and sales agreement with Prestige Capital Finance, LLC or Prestige Capital, pursuant to which Emmaus Medical may offer and sell to Prestige Capital from time to time eligible accounts receivable in exchange for Prestige Capital’s down payment, or advance, to Emmaus Medical of
At December 31, 2022 and 2021, accounts receivable included approximately $
Inventories—Inventories consist of raw materials, finished goods and work-in-process and are valued on a first‑in, first‑out basis at the lesser of cost or net realizable value. Work‑in‑process inventories consist of L‑glutamine for the Company’s products that has not yet been packaged and labeled for sale. Substantially all raw materials purchase during the years ended December 31, 2022 and 2021 were supplied, directly or indirectly by
Prepaid expenses and other current assets— Prepaid expenses and other current assets consist primarily of cost paid for future services or refunds from vendors which will occur within a year. Prepaid expenses include prepayment in insurance, subscription services, consulting and other services which are being amortized over the contract terms or recognized upon services are performed.
Property and equipment— Equipment, Furniture and fixtures are recorded at historical cost and amortized on a straight‑line basis over their estimated useful lives of to
F-11
Impairment of long‑lived assets—The Company evaluates the carrying value of its long‑lived assets for impairment whenever events or changes in circumstances indicate that such carrying values may not be recoverable. The Management uses its best judgment based on the current facts and circumstances relating to the Company’s business when determining whether any significant impairment factors exist.
If the Company determines that the carrying values of long‑lived assets may not be recoverable based upon the existence of one or more indicators of impairment, the Company performs an undiscounted cash flow analysis to determine if impairment exists. If impairment exists, the Company measures the impairment based on the difference between the asset’s carrying amount and its fair value, and the impairment is reflected in the consolidated statement of operations in the period in which the long‑lived asset impairment is determined to have occurred.
Research and development—Research and development consists of expenditures for the research and development of the Company’s products and product candidates, which primarily involve contract research, payroll‑related expenses and other related supplies. Research and development costs are expensed as incurred.
Share‑based compensation—The Company recognizes compensation cost for share‑based compensation awards over the service term of the recipients of the share‑based awards. The fair value of share‑based compensation is calculated using the Black‑Scholes‑Merton pricing model. The Black‑Scholes‑Merton model requires subjective assumptions regarding future stock price volatility and expected time to exercise, which greatly affect the calculated values. The expected term of awards granted is calculated using the simplified method allowed under the Securities and Exchange Commission (“SEC”) Staff Accounting Bulletin Nos. 107 and 110. The risk‑free rate selected to value any grant is based on the U.S. Treasury rate on the grant date that corresponds to the expected term of the award.
Income taxes—The Company accounts for income taxes under the asset and liability method, wherein deferred tax assets and liabilities are recognized for the future tax consequences attributable to the differences between the financial statement carrying amounts of existing assets and liabilities and their respective tax bases. Deferred tax assets and liabilities are measured using enacted tax rates expected to apply to taxable income in the years in which those temporary differences are expected to be recovered or settled. The effect on deferred tax assets and liabilities of a change in tax rates is recognized in income in the period the enactment occurs. A valuation allowance is provided for certain deferred tax assets if it is more likely than not that the Company will not realize tax assets through the generation of future taxable income for the related jurisdictions.
When tax returns are filed, it is highly probable that some positions taken would be sustained upon examination by the taxing authorities, while others are subject to uncertainty about the merits of the position taken or the amount of the position that would be ultimately sustained. The benefit of a tax position is recognized in the financial statements in the period during which, based on all available evidence, management believes it is more likely than not that the position will be sustained upon examination, including the resolution of appeals or litigation processes, if any. Tax positions taken are not offset or aggregated with other positions. Tax positions that meet the more‑likely‑than‑not recognition threshold are recorded at the largest amount of tax benefit that is more than 50 percent likely of being realized upon examination by the applicable taxing authority. The portion of the benefits associated with tax positions taken that exceeds the amount measured as described above is reflected as a liability for unrecognized tax benefits along with any associated interest and penalties that would be payable to the taxing authorities upon examination.
As of December 31, 2022 and 2021, the Company had
Comprehensive loss—Comprehensive loss includes net loss and other comprehensive loss relating to foreign translation adjustments of the Company’s subsidiaries and the changes in fair value of investment in convertible bond classified as available for sale.
Equity method investment – The Company owns
F-12
Investment in convertible bond – The Company has elected the fair value option measuring its investment in convertible bond. The convertible bond is classified as available for sale and the changes in fair value are reported in other comprehensive loss for each reporting period.
Foreign currency translation—The Company’s reporting currency is the U.S. dollar. The functional currencies of its foreign subsidiaries are the primary currencies within the counties in which they operate. Assets and liabilities of their operations are translated into U.S. dollars at period‑end exchange rates, and revenues, if any, and expenses are translated into U.S. dollars at average exchange rates in effect during each reporting period. Adjustments resulting from the translation are reported in other comprehensive loss.
Financial instruments—Financial instruments included in the financial statements are comprised of cash and cash equivalents, investment in convertible bond, accounts receivable, warrant derivative liabilities, accounts payable, certain accrued liabilities, convertible notes payable, notes payable, conversion feature liabilities and other contingent liabilities.
Fair value measurements—The Company defines fair value as the price that would be received to sell an asset or paid to transfer a liability in an orderly transaction between market participants at the measurement date in accordance with ASC 820. The Company measures fair value under a framework that provides a fair value hierarchy that prioritizes the inputs to valuation techniques used to measure fair value. The hierarchy gives the highest priority to unadjusted quoted prices in active markets for identical assets or liabilities (Level 1 measurements) and the lowest priority to unobservable inputs (Level 3 measurements). The three levels of the fair value hierarchy are described as follows:
Level 1: Inputs to the valuation methodology are unadjusted quoted prices for identical assets or liabilities in active markets.
Level 2: Inputs to the valuation methodology include:
Quoted prices for similar assets or liabilities in active markets;
Quoted prices for identical or similar assets or liabilities in inactive markets;
Inputs other than quoted prices that are observable for the asset or liability; and
Inputs that are derived principally from or corroborated by observable market data by correlation or other means.
If the asset or liability has a specified (contractual) term, the Level 2 inputs must be observable for substantially the full term of the asset or liability.
Level 3: Inputs to the valuation methodology are unobservable and significant to the fair value measurement.
The fair value measurement level of an asset or liability within the fair value hierarchy is based on the lowest level of any input that is significant to the fair value measurement. Valuation techniques used need to maximize the use of observable inputs and minimize the use of unobservable inputs. The carrying values of cash and cash equivalents, accounts receivables, other current assets, account payable and accrued expenses, other current liabilities and revolving line of credit approximate fair value due to the short-term maturity of those instruments. The fair value of the Company's convertible debt instruments was determined based on Level 2 inputs. The carrying value of the debt was discounted based on allocating proceeds to other financial instruments within the arrangement as discussed in Note 7.
Certain outstanding warrants contain price adjustment provisions and, consequently, are accounted for as liabilities that are remeasured at fair value on a recurring basis using Level 3 inputs. The level 3 inputs in the valuation of the warrants include expected term and expected volatility as discussed in Note 8. There are no other assets or liabilities measured at fair value on a recurring basis.
Net loss per share—In accordance with ASC 260, “Earnings per Share,” the basic net loss per common share is computed by dividing net loss available to common stockholders by the weighted-average number of common shares outstanding. Dilutive net loss per share is computed in a similar manner, except that the denominator is increased to include the number of additional common shares that would have been outstanding if the potential common shares had been issued and if the additional common shares were dilutive. As of December 31, 2022 and 2021, there were
F-13
Segment reporting—The Company operates in
Recent accounting pronouncements— Management has considered all recent accounting pronouncements and determined that they will not have a material effect on the Company’s consolidated financial statements.
NOTE 3—REVENUES, NET
Revenues, net by category were as follows (in thousands):
|
Years ended December 31, |
|
|||||
|
2022 |
|
|
2021 |
|
||
Endari® |
$ |
|
|
$ |
|
||
Other |
|
|
|
|
|
||
Revenues, net |
|
|
|
|
|
||
The following table summarizes the revenue allowance and accrual activities for the years ended December 31, 2022, and 2021 (in thousands):
|
|
Trade Discounts, Allowances and Chargebacks |
|
|
Government Rebates and Other Incentives |
|
|
Returns |
|
|
Total |
|
||||
Balance as of December 31, 2020 |
|
$ |
|
|
$ |
|
|
$ |
|
|
|
|
||||
Provision related to sales in the current year |
|
|
|
|
|
|
|
|
|
|
|
|
||||
Adjustments related to prior period sales |
|
|
|
|
|
|
|
|
( |
) |
|
|
|
|||
Credit and payments made |
|
|
( |
) |
|
|
( |
) |
|
|
( |
) |
|
|
( |
) |
Balance as of December 31, 2021 |
|
|
|
|
|
|
|
|
|
|
|
|
||||
Provision related to sales in the current year |
|
|
|
|
|
|
|
|
|
|
|
|
||||
Adjustments related to prior period sales |
|
|
( | ) |
|
|
|
|
|
|
|
|
|
|||
Credit and payments made |
|
|
( |
) |
|
|
( |
) |
|
|
( |
) |
|
|
( |
) |
Balance as of December 31, 2022 |
|
$ |
|
|
$ |
|
|
$ |
|
|
$ |
|
||||
The following table summarizes revenue attributable to each of the customers that accounted for 10% or more of net revenues in either of the period shown:
|
|
Years Ended December 31, |
|
|||||
|
|
2022 |
|
|
2021 |
|
||
Customer A |
|
|
% |
|
|
% |
||
Customer B |
|
|
% |
|
|
% |
||
Customer C |
|
|
% |
|
|
% |
||
Customer D |
|
|
% |
|
|
— |
|
|
The Company is a party to a distributor agreement with Telcon RF Pharmaceutical, Inc., or Telcon, pursuant to which it granted Telcon exclusive rights to the Company’s PGLG oral powder for the treatment of diverticulosis in South Korea, Japan and China in exchange for Telcon’s payment of a $
F-14
NOTE 4—SELECTED FINANCIAL STATEMENT ASSETS
Inventories consisted of the following (in thousand):
|
As of December 31 |
|
|||||
|
2022 |
|
|
2021 |
|
||
Raw materials and components |
$ |
|
|
$ |
|
||
Work-in-process |
|
|
|
|
|
||
Finished goods |
|
|
|
|
|
||
Inventory reserve |
|
( | ) |
|
|
( | ) |
Total inventories, net |
$ |
|
|
$ |
|
||
Prepaid expenses and other current assets consisted of the following (in thousands):
|
As of December 31 |
|
|||||
|
2022 |
|
|
2021 |
|
||
Prepaid insurance |
$ |
|
|
$ |
|
||
Prepaid expenses |
|
|
|
|
|
||
Other current assets |
|
|
|
|
|
||
Total prepaid expenses and other current assets |
$ |
|
|
$ |
|
||
Property and equipment consisted of the following (in thousands):
|
As of December 31 |
|
|||||
|
2022 |
|
|
2021 |
|
||
Equipment |
$ |
|
|
$ |
|
||
Leasehold improvements |
|
|
|
|
|
||
Furniture and fixtures |
|
|
|
|
|
||
Construction-in-progress |
|
— |
|
|
|
|
|
Total property and equipment |
|
|
|
|
|
||
Less: accumulated depreciation |
|
( |
) |
|
|
( |
) |
Total property and equipment, net |
$ |
|
|
$ |
|
||
NOTE 5 — INVESTMENTS
Investment in convertible bond - On September 28, 2020, the Company entered into a convertible bond purchase agreement pursuant to which it purchased at face value a convertible bond of Telcon in the principal amount of approximately $
Concurrent with the purchase of the convertible bond, the Company entered into an agreement dated
F-15
The Company has elected the fair value option method of accounting for the investment in convertible bond. The investment in convertible bond is classified as an available for sale security and remeasured at fair value on a recurring basis using Level 3 inputs, with any changes in the fair value option recorded in other comprehensive loss. The fair value and any changes in fair value in the convertible bond is determined using a binominal lattice model. The model produces an estimated fair value based on changes in the price of the underlying common stock over successive periods of time.
In February 2022, the Company and Telcon agreed to settle a “target shortfall” under the revised API agreement with Telcon for the years ended 2020 and 2021 by exchanging KRW
The following table sets forth the fair value and changes in fair value of the investment in the Telcon convertible bond as of December 31, 2022 and 2021 (in thousands):
Investment in convertible bonds |
|
December 31, 2022 |
|
|
December 31, 2021 |
|
||
Balance, beginning of period |
|
$ |
|
|
$ |
|
||
Sales of convertible bond |
|
|
( |
) |
|
|
— |
|
|
|
( |
) |
|
|
— |
|
|
|
|
( |
) |
|
|
( |
) |
|
Balance, end of period |
|
$ |
|
|
$ |
|
||
The fair values as of December 31, 2022 and December 31, 2021 were based upon following assumptions:
|
|
December 31, 2022 |
|
|
December 31, 2021 |
|
||
Principal outstanding (South Korean won) |
|
KRW |
|
|
KRW |
|
||
Stock price |
|
KRW |
|
|
KRW |
|
||
Expected life (in years) |
|
|
|
|
|
|
||
Selected yield |
|
|
% |
|
|
% |
||
Expected volatility (Telcon common stock) |
|
|
% |
|
|
% |
||
Risk-free interest rate (South Korea government bond) |
|
|
% |
|
|
% |
||
Expected dividend yield |
|
|
% |
|
|
% |
||
Conversion price |
|
KRW |
|
|
KRW |
|
||
Equity method investment – During 2018, the Company and Japan Industrial Partners, Inc., or JIP, formed EJ Holdings Inc., or EJ Holdings, to acquire, own and operate an amino acids manufacturing facility in Ube, Japan. In connection with the formation, the Company invested approximately $
EJ Holdings is engaged in seeking to refurbish and phase in the Ube facility with objective of eventually obtaining regulatory clearance for the manufacture of PGLG in accordance with cGMP. EJ Holdings has had no substantial revenues since its inception, has depended on loans from the Company to acquire the Ube facility and fund its operations and will continue to be dependent on loans from the Company or other financing unless and until its plant is activated and it can secure customers, including the Company, for its products. There is no assurance the Company can continue to provide needed funding EJ Holdings, or that needed funding will be available from other source. EJ Holdings has no commitments or understandings regarding any additional funding. If EJ Holdings fail to obtain needed funding, it may need to suspend
F-16
activities at the Ube plant. Under the asset purchase agreement by which EJ Holdings purchased the Ube plant, the seller has the right to repurchase the plant at the purchase price, plus certain taxes, paid by EJ Holdings if the plant does not become operational within a reasonable period of time (not to exceed five years). In such event, it is likely that the Company would lose some or all of its investment.
The Company has determined that EJ Holdings is a variable interest entity, or VIE, based upon its dependence on loan financing provided by the Company to acquire the Ube facility and to carry on EJ Holdings' activities and that the EJ Holdings’ activities, which are principally for the Company’s benefit. JIP, however, owns
The Company’s share of the losses reported by EJ Holdings are classified as net losses on equity method investment. The investment is evaluated for impairment if facts and circumstances indicate that the carrying value may not be recoverable, an impairment charge would be recorded.
The following table sets forth certain unaudited financial information of EJ Holdings as of December 31, 2022 and 2021 and for the 12 months ended December 31, 2022 and 2021 (in thousands):
|
As of December 31, |
|
|||||
|
2022 |
|
|
2021 |
|
||
ASSETS |
|
|
|
|
|
||
Current assets |
$ |
|
|
$ |
|
||
Other assets |
|
|
|
|
|
||
Total assets |
$ |
|
|
$ |
|
||
LIABILITIES |
|
|
|
|
|
||
Current liabilities |
$ |
|
|
$ |
|
||
Long-term liabilities |
|
|
|
|
|
||
Total liabilities |
$ |
|
|
$ |
|
||
Noncontrolling interest |
$ |
( |
) |
|
$ |
( |
) |
|
|
|
|
|
|
||
|
Years Ended December 31, |
|
|||||
|
2022 |
|
|
2021 |
|
||
Revenue, net |
$ |
|
|
$ |
|
||
Net loss |
$ |
( |
) |
|
$ |
( |
) |
F-17
NOTE 6—SELECTED FINANCIAL STATEMENT LIABILITIES
Accounts payable and accrued expenses as of December 31, 2022 and 2021 consisted of the following (in thousands):
|
|
December 31, 2022 |
|
|
December 31, 2021 |
|
||
Accounts payable: |
|
|
|
|
|
|
||
Clinical and regulatory expenses |
|
$ |
|
|
$ |
|
||
Professional fees |
|
|
|
|
|
|
||
Selling expenses |
|
|
|
|
|
|
||
Manufacturing costs |
|
|
|
|
|
|
||
Non-employee board member compensation |
|
|
|
|
|
|
||
Other vendors |
|
|
|
|
|
|
||
Total accounts payable |
|
|
|
|
|
|
||
Accrued interest payable, related parties |
|
|
|
|
|
|||
Accrued interest payable |
|
|
|
|
|
|
||
Accrued expenses: |
|
|
|
|
|
|
||
Payroll expenses |
|
|
|
|
|
|
||
Government rebates and other rebates |
|
|
|
|
|
|
||
Other accrued expenses |
|
|
|
|
|
|
||
Total accrued expenses |
|
|
|
|
|
|
||
Total accounts payable and accrued expenses |
|
$ |
|
|
$ |
|
||
Other current liabilities consisted of the following (in thousands):
|
As of December 31 |
|
|||||
|
2022 |
|
|
2021 |
|
||
Trade discount |
$ |
|
|
$ |
|
||
Unearned revenue |
|
|
|
|
— |
|
|
Other current liabilities |
|
|
|
|
|
||
Total other current liabilities |
$ |
|
|
$ |
|
||
Other long-term liabilities consisted of the following (in thousands):
|
As of December 31 |
|
|||||
|
2022 |
|
|
2021 |
|
||
Trade discount |
$ |
|
|
$ |
|
||
Unearned revenue |
|
— |
|
|
|
|
|
Other long-term liabilities |
|
|
|
|
|
||
Total other long-term liabilities |
$ |
|
|
$ |
|
||
On June 12, 2017, the Company entered into an API Supply Agreement with Telcon pursuant to which Telcon advanced to the Company approximately $
F-18
NOTE 7—NOTES PAYABLE
Notes payable consisted of the following at December 31, 2022 and 2021 (in thousands except for conversion price and underlying shares) excluding the revolving line of credit agreement with related party discussed below:
Year |
|
Interest Rate |
|
Term of Notes |
|
Conversion |
|
|
Principal |
|
|
Unamortized Discount December 31, 2022 |
|
|
Carrying |
|
|
Shares |
|
|||||
Notes payable |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
2013 |
|
|
|
|
— |
|
|
$ |
|
|
$ |
— |
|
|
$ |
|
|
|
— |
|
||||
2021 |
|
|
|
|
— |
|
|
|
|
|
|
— |
|
|
|
|
|
|
— |
|
||||
2022 |
|
|
|
|
— |
|
|
|
|
|
|
|
|
$ |
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
$ |
|
|
$ |
|
|
$ |
|
|
|
— |
|
||||
|
|
|
|
Current |
|
|
|
|
$ |
|
|
$ |
|
|
$ |
|
|
|
— |
|
||||
|
|
|
|
Non-current |
|
|
|
|
$ |
|
|
$ |
|
|
$ |
|
|
|
— |
|
||||
Notes payable - related parties |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
2020 |
|
|
|
|
— |
|
|
|
|
|
|
— |
|
|
|
|
|
|
— |
|
||||
2021 |
|
|
|
|
— |
|
|
|
|
|
|
— |
|
|
|
|
|
|
— |
|
||||
2022 |
|
|
|
|
— |
|
|
|
|
|
|
|
|
|
|
(c) |
|
— |
|
|||||
|
|
|
|
|
|
|
|
|
$ |
|
|
$ |
|
|
$ |
|
|
|
— |
|
||||
|
|
|
|
Current |
|
|
|
|
$ |
|
|
$ |
— |
|
|
$ |
|
|
|
— |
|
|||
|
|
|
|
Non-current |
|
|
|
|
$ |
|
|
$ |
|
|
$ |
|
|
|
— |
|
||||
Convertible notes payable |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
2020 |
|
|
|
$ |
|
(a) |
|
|
|
|
— |
|
|
|
|
|
|
|
||||||
2021 |
|
|
|
$ |
|
(b) |
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
$ |
|
|
$ |
|
|
$ |
|
|
|
|
|||||
|
|
|
|
Current |
|
|
|
|
$ |
|
|
$ |
|
|
$ |
|
|
|
|
|||||
|
|
|
|
Grand Total |
|
|
|
|
$ |
|
|
$ |
|
|
$ |
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Year |
|
Interest Rate |
|
Term of Notes |
|
Conversion |
|
|
Principal |
|
|
Unamortized |
|
|
Carrying |
|
|
Shares |
|
|||||
Notes payable |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
2013 |
|
|
|
|
— |
|
|
$ |
|
|
$ |
— |
|
|
$ |
|
|
|
— |
|
||||
2021 |
|
|
|
|
— |
|
|
|
|
|
|
— |
|
|
|
|
|
|
— |
|
||||
|
|
|
|
|
|
|
|
|
$ |
|
|
$ |
— |
|
|
$ |
|
|
|
— |
|
|||
|
|
|
|
Current |
|
|
|
|
$ |
|
|
$ |
— |
|
|
$ |
|
|
|
— |
|
|||
|
|
|
|
Non-current |
|
|
|
|
$ |
|
|
$ |
— |
|
|
$ |
|
|
|
— |
|
|||
Notes payable - related parties |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
2020 |
|
|
|
|
— |
|
|
|
|
|
|
— |
|
|
|
|
|
|
— |
|
||||
2021 |
|
|
|
|
— |
|
|
|
|
|
|
— |
|
|
|
|
|
|
— |
|
||||
|
|
|
|
|
|
|
|
|
$ |
|
|
$ |
— |
|
|
$ |
|
|
|
— |
|
|||
|
|
|
|
Current |
|
|
|
|
$ |
|
|
$ |
— |
|
|
$ |
|
|
|
— |
|
|||
Convertible notes payable |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
2020 |
|
|
|
$ |
|
(a) |
|
|
|
|
— |
|
|
|
|
|
|
|
||||||
2021 |
|
|
|
$ |
|
(b) |
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
$ |
|
|
$ |
|
|
$ |
|
|
|
|
|||||
|
|
|
|
Current |
|
|
|
|
$ |
|
|
$ |
|
|
$ |
|
|
|
|
|||||
|
|
|
|
Non-current |
|
|
|
|
$ |
|
|
$ |
— |
|
|
$ |
|
|
|
|
||||
|
|
|
|
Grand Total |
|
|
|
|
$ |
|
|
$ |
|
|
$ |
|
|
|
|
|||||
The weighted-average stated interest rate of notes payable was
F-19
As of December 31, 2022, future contractual principal payments due on notes payable were as follows (in thousands):
Year Ending |
|
|
|
2023 |
|
|
|
2024 |
|
|
|
2025 |
|
— |
|
2026 |
|
— |
|
2027 |
|
|
|
Total |
$ |
|
|
The Company is party to a revolving line of credit agreement with Yutaka Niihara., M.D., M.P.H., the Company’s Chairman and Chief Executive Officer. Under the agreement, at the Company’s request from time to time, Dr. Niihara may, but is not obligated to, loan or re-loan to the Company up to $
On February 9, 2021, the Company entered into a securities purchase agreement pursuant to which the Company agreed to sell and issue to the purchasers thereunder in a private placement pursuant to Rule 4(a)(2) of the Securities Act of 1933, as amended, and Regulation D thereunder a total of up to $
Commencing one year from the original issue date, the convertible promissory notes became convertible at the option of the holder into shares of the Company’s common stock at an initial conversion price of $
The conversion feature of the convertible promissory notes is separately accounted for at fair value as a derivative liability under guidance in ASC 815 that is remeasured at fair value on a recurring basis using Level 3 inputs, with any changes in the fair value of the conversion feature liability recorded in the statements of operations.
Convertible promissory notes |
|
December 31, 2022 |
|
|
December 31, 2021 |
|
||
Balance, beginning of period |
|
$ |
|
|
$ |
— |
|
|
Fair value at issuance date |
|
|
— |
|
|
|
|
|
|
|
( |
) |
|
|
|
||
Balance, end of period |
|
$ |
|
|
$ |
|
||
The fair value and any change in fair value of conversion feature liability are determined using a binomial lattice model. The model produces an estimated fair value based on changes in the price of the underlying common stock.
F-20
The fair value as of December 31, 2022 and December 31, 2021 was based on upon following assumptions:
Convertible promissory notes |
|
December 31, 2022 |
|
|
December 31, 2021 |
|
||
Stock price |
|
$ |
|
|
$ |
|
||
Conversion price |
|
$ |
|
|
$ |
|
||
Select yield |
|
|
% |
|
|
% |
||
Expected volatility |
|
|
% |
|
|
% |
||
Time until maturity (in years) |
|
|
|
|
|
|
||
Dividend yield |
|
— |
|
|
— |
|
||
Risk-free rate |
|
|
% |
|
|
% |
||
In June 2022, the Company entered into a Business Loan and Security Agreement and Addenda with a third-party lender pursuant to which the lender loaned the Company $
In July 2022, Dr. Niihara and his wife loaned the Company $
In August 2022, Dr. Niihara and his wife loaned the Company $
In September 2022, Seah Lim, M.D., Ph.D. loaned the Company $
In July 2022, Emmaus Medical, Inc., or Emmaus Medical, an indirect wholly owned subsidiary of the Company, entered into a Standard Merchant Cash Advance Agreement with a third party pursuant to which it sold $
F-21
and the obligations of Emmaus Medical and the guarantors are secured by a security interest in all or substantially all the assets of Emmaus Life Sciences and its U.S. subsidiaries. In December 2022, both loans were repaid in full and recognized debt extinguishment loss of $
In December 2022, the Company entered an Agreement for the Purchase and Sales of Future Receipts with a third party pursuant to which it sells $
NOTE 8—STOCKHOLDERS’ DEFICIT
Purchase agreement with Holder of a Convertible Promissory Note — On June 15, 2020, the holder of a convertible promissory note in the principal amount of $
The following table presents the change in fair value of the warrants as of June 15, 2022 and 2021 (in thousands):
Warrant liability— Convertible Promissory Note |
|
June 15, 2022 |
|
|
December 31, 2021 |
|
||
Balance, beginning of period |
|
$ |
|
|
$ |
|
||
|
|
( |
) |
|
|
|
||
Reclassification to equity |
|
|
( |
) |
|
|
— |
|
Balance, end of period |
|
$ |
— |
|
|
$ |
|
|
The fair value of the warrant derivative liabilities was determined using the Black-Scholes Merton model and was based upon following assumptions:
|
|
June 15, 2022 |
|
|
December 31, 2021 |
|
||
Exercise price |
|
$ |
|
|
$ |
|
||
Stock price |
|
$ |
|
|
$ |
|
||
Risk‑free interest rate |
|
|
% |
|
|
% |
||
Expected volatility (peer group) |
|
|
% |
|
|
% |
||
Expected life (in years) |
|
|
|
|
|
|
||
Expected dividend yield |
|
— |
|
|
— |
|
||
Number outstanding |
|
|
|
|
|
|
||
A summary of the Company’s warrants activity for the years ended December 31, 2022 and 2021 is presented below:
|
December 31, 2022 |
|
|
December 31, 2021 |
|
||||||||||
|
Number of Warrants |
|
|
Weighted |
|
|
Number of Warrants |
|
|
Weighted |
|
||||
Warrants outstanding, beginning of period |
|
|
|
$ |
|
|
|
|
|
$ |
|
||||
Granted |
|
|
|
$ |
|
|
|
— |
|
|
$ |
— |
|
||
Exercised |
|
— |
|
|
$ |
— |
|
|
|
— |
|
|
$ |
— |
|
Cancelled, forfeited and expired |
|
( |
) |
|
$ |
|
|
|
( |
) |
|
$ |
|
||
Warrants outstanding, end of period |
|
|
|
$ |
|
|
|
|
|
$ |
|
||||
Warrant exercisable, end of period |
|
|
|
$ |
|
|
|
|
|
$ |
|
||||
F-22
Warrants — In September 2022, in connection with the loans from Dr. Niihara and his wife, the Company granted Dr. Niihara a
As of December 31, 2022, the weighted-average remaining contractual life of outstanding warrants was
Stock options — Upon completion of the Merger, the EMI Holding Amended and Restated 2011 Stock Incentive Plan was assumed by the Company. The 2011 Stock Incentive Plan permits grants of incentive stock options to employees, including executive officers, and other share-based awards such as stock appreciation rights, restricted stock, stock units, stock bonus and unrestricted stock awards to employees, directors, and consultants for up to
The Company also had an Amended and Restated 2012 Omnibus Incentive Compensation Plan under which the Company may grant incentive stock options to selected employees including officers, non-employee consultants and non-employee directors. The Plan was terminated in September 2021.
On September 29, 2021, the Board of Directors of the Company adopted the Emmaus Life Sciences, Inc. 2021 Stock Incentive Plan upon the recommendation of the Compensation Committee of the Board. The 2021 Stock Incentive Plan was approved by stockholders on November 23, 2021. No more than
Management has valued stock options at their date of grant utilizing the Black‑Scholes‑Merton Option pricing model. The fair value of the underlying shares was determined by the market value of stock of similar companies and recent arm’s length transactions involving the sale of the Company’s common stock. Prior the Merger, the Company lacked company-specific historical and implied volatility information for its common stock. Therefore, the expected volatility was calculated using the historical volatility of a comparative public traded companies. The following table presents the assumptions used on recent dates on which options were granted by the Company.
The risk‑free interest rate is based on the implied yield available on U.S. Treasury issues with a term approximating the expected life of the options depending on the date of the grant and expected life of the respective options.
A summary of the Company’s stock option activity for the years ended December 31, 2022 and 2021 is presented below:
|
|
December 31, 2022 |
|
|
December 31, 2021 |
|
||||||||||
|
|
Number of |
|
|
Weighted‑ |
|
|
Number of |
|
|
Weighted‑ |
|
||||
Options outstanding, beginning of period |
|
|
|
|
$ |
|
|
|
|
|
$ |
|
||||
Granted or deemed issued |
|
|
— |
|
|
$ |
— |
|
|
|
— |
|
|
$ |
— |
|
Exercised |
|
|
— |
|
|
$ |
— |
|
|
|
— |
|
|
$ |
— |
|
Cancelled, forfeited and expired |
|
|
( |
) |
|
$ |
|
|
|
( |
) |
|
$ |
|
||
Options outstanding, end of period |
|
|
|
|
$ |
|
|
|
|
|
$ |
|
||||
Options exercisable at end of year |
|
|
|
|
$ |
|
|
|
|
|
$ |
|
||||
Options available for future grant |
|
|
|
|
|
|
|
|
|
|
|
|
||||
During the years ended December 31, 2022 and 2021, the Company recognized $
F-23
compensation cost related to unvested share‑based compensation awards outstanding under the EMI Amended and Restated 2011 Stock Incentive Plan. That cost is expected to be recognized over the weighted-average remaining period of
Collaborative Research and Development Agreement with Kainos Medicine, Inc—On February 26, 2021, the Company entered into a collaborative and research and development agreement with Kainos Medicine, Inc. (“Kainos”) to lead the preclinical development of Kainos’ patented IRAK4 inhibitor (“KM10544”) as an anti-cancer drug and further advance the research and development activity currently underway at Kainos. The companies also entered into a letter of intent regarding possible future joint development of small molecule therapeutics and other pharmaceutical assets.
Pursuant to the agreement, the Company paid and issued to Kainos $
On October 7, 2021, the Company entered into a License Agreement, with Kainos under which Kainos granted the Company an exclusive license in the territory encompassing the U.S., the U.K. and the EU to patent rights, know-how and other intellectual property relating to Kainos’s novel IRAK4 inhibitor, referred to as KM10544, for the treatment of cancers, including leukemia, lymphoma and solid tumor cancers. In consideration of the license, the Company paid Kainos a six-figure upfront fee in cash and agreed to make additional cash payments upon the achievement of specified milestones totaling in the mid-eight figures and pay a single-digit percentage royalty based on net sales of the licensed products and a similar percentage of any sublicensing consideration.
During the year ended December 31, 2021, the Company incurred $
Amended and Restated Warrants – The Company evaluated its outstanding amended and restated warrants to purchase up to
In June 2022, the exercise price of outstanding amended and restated warrants was reduced to $
Stock issued for services – In June 2022, the Company issued
In December 2022, the Company issued
NOTE 9—INCOME TAXES
The provision for income taxes consists of the following for the years ended December 31, 2022 and 2021 (in thousands):
|
|
2022 |
|
|
2021 |
|
||
Current U.S. |
|
$ |
|
|
$ |
|
||
International |
|
|
|
|
|
— |
|
|
Deferred U.S. |
|
|
— |
|
|
|
— |
|
International |
|
|
— |
|
|
|
— |
|
|
|
$ |
|
|
$ |
|
||
F-24
Deferred tax assets consisted of the following as of December 31, 2022 and 2021 (in thousands):
|
|
2022 |
|
|
2021 |
|
||
Net operating loss carryforward |
|
$ |
|
|
$ |
|
||
General business tax credit |
|
|
|
|
|
|
||
Stock options |
|
|
|
|
|
|
||
Charitable contribution |
|
|
|
|
|
|
||
Accrued expenses |
|
|
|
|
|
|
||
Unearned revenue |
|
|
|
|
|
|
||
Allowance for bad debt |
|
|
|
|
|
|
||
Unrealized gain on foreign exchange translation and others |
|
|
|
|
|
|
||
Section 174 Expenditures |
|
|
|
|
|
— |
|
|
Unrealized gain/ (loss) on LT investment |
|
|
|
|
|
|
||
Other |
|
|
|
|
|
|
||
Total gross deferred tax assets |
|
|
|
|
|
|
||
Less valuation allowance |
|
|
( |
) |
|
|
( |
) |
Net deferred tax assets |
|
$ |
|
|
$ |
|
||
Deferred tax liabilities consisted of the following as of December 31, 2022 and 2021 (in thousands):
|
|
2022 |
|
|
2021 |
|
||
Unrealized gain on available-for-sale securities |
|
$ |
( |
) |
|
$ |
( |
) |
Other |
|
|
( |
) |
|
|
( |
) |
Total deferred tax liabilities |
|
$ |
( |
) |
|
$ |
( |
) |
A valuation allowance for the net deferred tax assets is recorded when it is more likely than not that the Company will not realize these assets through future operations. The valuation allowance increased by approximately $
As of December 31, 2022 and December 31, 2021, the Company had net operating loss carryforwards for federal income tax purposes of approximately $
The income tax provision differs from that computed using the statutory federal tax rate of
|
|
2022 |
|
|
2021 |
|
||
Tax benefit at statutory federal rate |
|
$ |
( |
) |
|
$ |
( |
) |
State taxes, net of federal tax benefit |
|
|
( |
) |
|
|
( |
) |
Increase (decreases) in valuation allowance |
|
|
|
|
|
|
||
Permanent items |
|
|
( |
) |
|
|
|
|
General business tax credit |
|
|
( |
) |
|
|
( |
) |
Other |
|
|
( |
) |
|
|
|
|
|
|
$ |
|
|
$ |
|
||
As of December 31, 2022 and December 31, 2021, the Company had no unrecognized tax benefits or position which, in the opinion of management, would be reversed if challenged by a taxing authority. In the event the Company is assessed interest or penalties, such amounts would be classified as income tax expense. As of December 31, 2022, all federal tax returns since 2019 are subject to audit. The expiration of the state returns varies by state, but the 2018 and subsequent years’ returns generally are subject to audit. No tax returns are currently being examined by taxing authorities.
F-25
NOTE 10—LEASES
Operating leases — During the years ended December 31, 2022 and 2021, the Company leased its office space under operating leases with unrelated entities.
The Company leased
Rent expense was $
Future minimum lease payments were as follows as of December 31, 2022 (in thousands):
|
|
Amount |
|
|
2023 |
|
|
|
|
2024 |
|
|
|
|
2025 |
|
|
|
|
2026 and thereafter |
|
|
|
|
Total lease payments |
|
|
|
|
Less: Interest |
|
|
( | ) |
Operating lease liabilities |
|
$ |
|
|
As of December 31, 2022 and 2021, the Company had an operating lease right-of-use asset of $
NOTE 11—COMMITMENTS AND CONTINGENCIES
API Supply Agreement — On June 12, 2017, the Company entered into an API Supply Agreement (the “API Agreement”) with Telcon pursuant to which Telcon paid the Company approximately $
F-26
NOTE 12—RELATED PARTY TRANSACTIONS
The following table sets forth information relating to our loans from related persons outstanding at any time during the year ended December 31, 2022 (in thousands except for conversion rate and share information):
Class |
Lender |
|
Interest |
|
Date of |
|
Term of Loan |
|
Principal Amount Outstanding December 31, 2022 |
|
|
Highest |
|
|
Amount of |
|
|
Amount of |
|
||||
Current, Promissory note payable to related parties: |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
Willis Lee(2) |
|
|
|
|
|
|
|
|
|
|
|
— |
|
|
|
— |
|
|||||
|
Soomi Niihara(1) |
|
|
|
|
|
|
|
|
|
|
|
— |
|
|
|
— |
|
|||||
|
Soomi Niihara(1) |
|
|
|
|
|
— |
|
|
|
|
|
|
|
|
|
|
||||||
|
Yasushi Nagasaki(2) |
|
|
|
|
|
— |
|
|
|
|
|
|
|
|
|
|
||||||
|
Hope International Hospice, Inc.(1) |
|
|
|
|
|
|
|
|
|
|
|
— |
|
|
|
— |
|
|||||
|
Hope International Hospice, Inc.(1) |
|
|
|
|
|
|
|
|
|
|
|
— |
|
|
|
— |
|
|||||
|
Soomi Niihara(1) |
|
|
|
|
|
|
|
|
|
|
|
— |
|
|
|
— |
|
|||||
|
George Sekulich(2) |
|
|
|
|
|
— |
|
|
|
|
|
|
|
|
|
|
||||||
|
Soomi Niihara(1) |
|
|
|
|
|
— |
|
|
|
|
|
|
|
|
|
|
||||||
|
Hope International Hospice, Inc.(1) |
|
|
|
|
|
|
|
|
|
|
|
— |
|
|
|
— |
|
|||||
|
Hope International Hospice, Inc.(1) |
|
|
|
|
|
|
|
|
|
|
|
— |
|
|
|
— |
|
|||||
|
Wei Peu Derek Zen(2) |
|
|
|
|
|
|
|
|
|
|
|
— |
|
|
|
— |
|
|||||
|
Willis Lee(2) |
|
|
|
|
|
|
|
|
|
|
|
— |
|
|
|
— |
|
|||||
|
Hope International Hospice, Inc.(1) |
|
|
|
|
|
|
|
|
|
|
|
— |
|
|
|
— |
|
|||||
|
Yutaka and Soomi Niihara(1) |
|
|
|
years |
|
|
|
|
|
|
|
|
— |
|
|
|
|
|||||
|
Hope International Hospice, Inc.(1) |
|
|
|
|
|
|
|
|
|
|
|
— |
|
|
|
— |
|
|||||
|
Yutaka and Soomi Niihara(1) |
|
|
|
years |
|
|
|
|
|
|
|
|
— |
|
|
|
|
|||||
|
Yutaka and Soomi Niihara(1) |
|
|
|
years |
|
|
|
|
|
|
|
|
— |
|
|
|
|
|||||
|
Hope International Hospice, Inc.(1) |
|
|
|
|
|
|
|
|
|
|
|
— |
|
|
|
— |
|
|||||
|
Yutaka and Soomi Niihara(1) |
|
|
|
|
|
|
|
|
|
|
|
— |
|
|
|
— |
|
|||||
|
Seah Lim(2) |
|
|
|
years |
|
|
|
|
|
|
|
|
— |
|
|
|
— |
|
||||
|
Hope International Hospice, Inc. |
|
|
|
|
|
|
|
|
|
|
|
— |
|
|
|
— |
|
|||||
|
|
|
|
|
|
|
Subtotal |
|
$ |
|
|
$ |
|
|
$ |
|
|
$ |
|
||||
Revolving line of credit agreement |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
Yutaka Niihara(2) |
|
|
|
|
|
— |
|
|
|
|
|
|
— |
|
|
|
|
|||||
|
|
|
|
|
|
|
Subtotal |
|
$ |
— |
|
|
$ |
|
|
$ |
— |
|
|
$ |
|
||
|
|
|
|
|
|
|
Total |
|
$ |
|
|
$ |
|
|
$ |
|
|
$ |
|
||||
F-27
The following table sets forth information relating to our loans from related persons outstanding at any time during the year ended December 31, 2021 (in thousands except for conversion rate and share information):
Class |
Lender |
|
Interest |
|
Date of |
|
Term of Loan |
|
Principal Amount Outstanding December 31, 2021 |
|
|
Highest |
|
|
Amount of |
|
|
Amount of |
|
||||
Current, Promissory note payable to related parties: |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
Willis Lee (2) |
|
|
|
|
$ |
|
|
$ |
|
|
$ |
— |
|
|
$ |
— |
|
|||||
|
Soomi Niihara (1) |
|
|
|
|
|
— |
|
|
|
|
|
|
|
|
|
|
||||||
|
Soomi Niihara (1) |
|
|
|
|
|
— |
|
|
|
|
|
|
|
|
|
|
||||||
|
Soomi Niihara (1) |
|
|
|
|
|
|
|
|
|
|
|
— |
|
|
|
— |
|
|||||
|
|
|
|
|
|
|
Subtotal |
|
$ |
|
|
$ |
|
|
$ |
|
|
$ |
|
||||
Revolving line of credit |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
Yutaka Niihara (1) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
Subtotal |
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
Total |
|
$ |
|
|
$ |
|
|
$ |
|
|
$ |
|
||||
(1) Dr. Niihara, a Director and the Chairman, and Chief Executive Officer of the Company, is also a director and the Chief Executive Officer of Hope International Hospice, Inc.
(2) Officer or director.
(3) The rate varies with changes in the prime rate and does not give effect to the “tax gross-up” described in Note 7.
See Note 7 for a discussion of the Company’s revolving line of credit agreement with Dr. Niihara and Note 8 for a discussion of the amendment to the previously issued warrant to Dr. Niihara.
See Notes 6 and 11 for a discussion of the Company’s distribution and supply agreements with Telcon, which holds
NOTE 13—DEFINED CONTRIBUTION PLAN
The Company has a defined contribution plan (the “401(k) Plan”) covering substantially all the Company’s employees. The Emmaus 401(k) Plan is a tax-qualified retirement saving plan, pursuant to which covered employees are able to contribute the lesser of
For the years ended December 31, 2022 and 2021, the Company made matching contributions to the Company’s 401(k) Plan of $
NOTE 14—SUBSEQUENT EVENTS
Subsequent to December 31, 2022, the Company received net proceeds of $
F-28